Liver Transplant Evaluation and Assessment Guide Guide
Welcome to the Queensland Liver Transplant Service (QLTS). The information in this guide will help you understand the process once your doctor has referred you to be considered for a liver transplant.
The first step of the workup is provided by the Hepatology Team at Burke Street outpatient clinic and/or in Ward 4E.
The evaluation process for a liver transplant is very thorough. We will be asking that you have many tests assessing the function of your liver and other important body organs. All test results are reviewed and may turn up new diagnoses which in turn may need further investigation. Test results will be discussed with you. Transplantation is not the treatment of choice for everyone.
Most patients have their transplant assessment as an outpatient. All the investigations are booked as outpatient appointments. For some patients it may be necessary for you to be admitted, and we will try to do as many tests as possible during your inpatient stay. The liver transplant coordinator will discuss with you how your assessment will be carried out.
Information and contact details for the liver transplant hepatology team
The pre-liver transplant clinic is located within the Hepatology Outpatient Clinics, located on the ground floor, Burke Street Centre every Wednesday 8.30 to 10am.
The liver - its function and anatomy
Liver function is essential to life. The liver performs a variety of very important functions and has the ability to repair itself.
It has a considerable reserve but there are many illnesses that lead to gradual damage and deterioration of the liver’s functions. Once the deterioration has continued to the point where there is not enough healthy tissue available to support the normal bodily functions, treatment options need to be considered. Transplantation is one option that will return an improved quality of life.
Common indications for liver transplantation include:
Cirrhosis due to chronic viral hepatitis for example Hepatitis B or C infection
Alcohol related liver disease
Fatty liver disease
Hepatocellular carcinoma
Autoimmune liver diseases including autoimmune hepatitis, primary sclerosing cholangitis and primary biliary cholangitis
Liver failure due to severe drug reactions
Inherited causes of liver disease and some metabolic disorders.
More information on your liver condition will be available from your treating doctor.
Liver functions
The liver has many important roles in keeping the body functioning.
Production of bile and bile salts. These help in the digestion and absorption of fats, fat-soluble vitamins and calcium salts.
Metabolism of carbohydrates, proteins and fats
Storage of glycogen, Vitamins A, D and B12, iron, lipids and cholesterol.
Production of some blood products, albumin and clotting factors
Metabolism or breakdown of various drugs and chemicals that would be harmful to the body.
When the liver is no longer able to complete these roles properly, we start to see complications of liver failure.
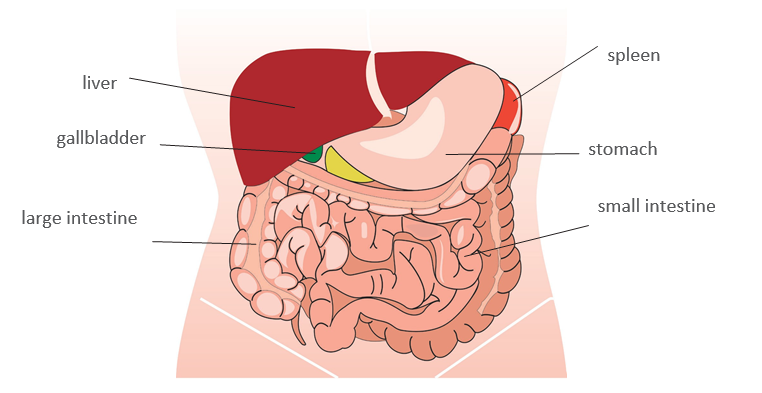
Anatomy
This diagram will assist you to have a better understanding of where the organs are located in the abdomen.
Signs of liver disease
We aim to help you manage your symptoms due to liver disease. We are here to support you, your family and significant others. Please ask members of the transplant team if you have any concerns. It is better to ask questions even if they seem minor, rather than worry about them, as the answer to your question may be very simple.
When the liver does not work properly, you may develop one or more symptoms or signs of liver failure.
Jaundice
Jaundice is when bilirubin accumulates in the blood. The skin and or the whites of your eyes appear yellow or greenish yellow due to high levels of the bile pigment. You may also become very itchy when you are jaundiced.
The itch associated with jaundice may be helped by:
Bathing using non fragrant soaps, try sorbolene or dove
Application of urea based skin creams to keep the skin moist
Wearing cotton clothes and avoiding synthetic materials
In some patients the doctor may start you on medications
Bleeding
Bleeding from the gums and easy bruising are frequently seen in patients with liver disease. Bleeding and or easy bruising is often due to minimal trauma in the presence of low platelet count.
Tips to minimise bleeding problems
Use an electric razor to shave
Use a soft toothbrush and avoid brushing too hard
Blow your nose gently
Portal hypertension
Portal hypertension is high blood pressure in the hepatic portal system—made up of the portal vein and its branches that drain from most of the intestine to the liver. If the vessels in the liver are blocked due to liver damage or scarring then blood cannot flow properly through the liver. This increased pressure in the portal vein may lead to the development of large, swollen veins also known as varices within the oesophagus, stomach, rectum, or umbilical area or belly button. Varices can rupture and bleed, resulting in potentially life-threatening complications.
Internal bleeding affects many people, so it is important to know the signs of bleeding:
Sudden fullness of the stomach
Becoming more tired
Blood stained or “coffee ground” vomiting
Black bowel movement or red blood in your bowel movement
Please seek medical advice if you have any of the above symptoms
Salt and fluid retention
Salt and fluid retention are common signs of liver failure and are due to the damaged liver no longer able to get rid of salt from the body, as well as low protein levels and disturbed kidney function. Retaining of salt can cause swollen ankles and ascites or fluid in the abdomen.
Treatment includes:
Low salt and high protein diet
Medications called diuretics or fluid tablets
Paracentesis or drainage of fluid from the abdomen
Hepatic encephalopathy
Hepatic encephalopathy is a condition which affects the brain. It can develop when the liver is damaged and unable to remove toxins, including ammonia from your blood.
Encephalopathy can present in several ways including:
Memory loss
Personality changes
Concentration and sleeping pattern changes
Confusion
Infections, some medications and constipation can cause episodes of encephalopathy. Sedatives or sleeping tablets can make the symptoms worse.
This condition can be very distressing to you and your family. Up to 70 per cent of patients with liver failure may have encephalopathy. In some cases, you may have to stop working and may have to stop driving. Your doctor will advise you if you have to stop driving, for your own safety and that of others on the road.
If this confusion occurs at home, please seek medical advice quickly
Ammonia
Bacteria in the intestine act on urea and protein to produce ammonia. Ammonia is cleared from the blood by a healthy liver. To help clear the ammonia from the body, patients are given Lactulose, a sweet liquid laxative which works by flushing out the ammonia in the intestine and decreasing the levels of bacteria in the bowel. The dose of lactulose is adjusted so that you are passing 2 to 3 soft bowel motions a day.
Do not take sleeping medication
Muscle wasting
Muscle wasting is common in patients with liver disease, and can result in weakness, loss of function and can make it more difficult to get through a transplant operation. It is important that we monitor your weight, muscle strength and fitness. You can help preserve your muscle mass by eating well – having small and regular meals, following a high protein diet and including a snack before bed. The dietitian will advise you of any supplements or dietary restrictions you need.
If you have been admitted to hospital for your assessment, and there are particular foods you like, a relative or friend is welcome to bring them in.
Exercise
You are encouraged to keep active and fit before your transplant. This is important because being unfit and losing muscle mass is linked to more health problems both before and after your liver transplant and can impact on your ability to get through and recover from surgery.
Aerobic exercises for example walking, cycling or swimming are good for your fitness levels and muscle function, and resistance and strength exercises, for example weights, help maintain your muscle mass and strength. When you come to clinic, your doctor and dietitian will speak to you about exercise. If you do not feel safe to exercise, or have concerns, you can speak to your general practitioner about being referred to an Exercise Physiologist in the community.
Nutritional problems
Inability to absorb and process vitamins and minerals can occur in liver disease. The levels of essential vitamins and minerals in your blood will be checked, and you will be advised if you need to take supplements.
Alcohol and smoking
Continuing to smoke or drink alcohol will prevent you from being considered for a liver transplant. If you are having problems avoiding alcohol or quitting smoking please ask for help as we have several programs available.
Pre-transplant assessment and evaluation
As you are being considered for liver transplantation, a complete evaluation of all your body systems must be done in order to determine the extent of your disease and make sure that you don’t have any other major health problems that prevent you from having a liver transplant.
The evaluation consists of many laboratory tests, hepatology and radiology procedures as well as check ups with other specialists. These check ups will be requested according to your individual medical needs.
In order to help you become familiar with various medical words and terms, explanations can be found throughout this booklet. Descriptions of many diagnostic procedures can be found in the glossary.
The assessment team
We fully appreciate that this can be a daunting time for you, your family and friends, so please do not hesitate to ask questions. Many professionals are involved in your care and are happy to help.
The members of our team include specialist doctors: hepatologists, hepatobiliary and liver transplant surgeons and anaesthetists. Depending on your medical needs, specialist reviews by alcohol and addiction specialists, psychiatry, renal, cardiology, respiratory, endocrine or palliative care may be necessary. The social worker, dietician, dentist, physiotherapist, pharmacist, pastoral care and liver transplant recipient coordinator will also see you during your evaluation. You will be given specialised information from many of these professionals.
Allied Health Services
Social worker
The social workers within the hepatology and liver transplant team can provide support at all stages of the assessment and treatment process to patients and families. This occurs through general discussion, shared information, counselling, education, and referral to other services. When referred to the Princess Alexandra Hospital for liver transplant assessment, an information package including a Social Work Intake Questionnaire is sent to all patients and their families by the liver transplant coordinators. This Questionnaire provides opportunity for patients and families to tell us about their life situation. A telehealth, usually by phone or in-person, social work clinic appointment occurs soon after the Questionnaire has been returned. This assists us to work out with you and your family what information and support would be most useful at this time.
Having been told they may need a liver transplant, many patients and families describe feeling anxious or overwhelmed as the prospect of a transplant is a totally new experience for them. There can be uncertainty about many things. Concerns and questions often centre around where to stay, how to manage income and expenses or how to address advance care planning and legal matters, for example, an Enduring Power of Attorney, Will, and an Advance Health Care Directive or Metro South Statement of Choices.
Often patients are worried about how their family members, especially young children; might be feeling and coping. For many people, preparing and waiting for a liver transplant can contribute towards changed family and personal relationships, employment, day to day activities and place of residence, you may need to move to Brisbane.
There is often much anticipation around the possibility of receiving a liver transplant, yet grief and worry that the liver is failing and the patient is getting sicker. It can be very tough on everyone in the family. The social worker can provide support and care throughout this time to patients and their families.
The transplant process is physically, medically, emotionally and personally demanding; therefore clear criteria must be met to be placed onto the waiting list for a transplant. Even though transplantation is a well-known treatment with stories about organ donation and transplants often featuring in mainstream and social media; unfortunately, it is not for everyone. If the team is unable to list you for a transplant, your options will be sensitively and carefully discussed with you and your family.
Patients and families are very welcome to make an appointment with the social worker at any stage of the treatment process for information, support, counselling or referral to another support service.
The transplant dietitian will provide a complete nutritional assessment. This is to determine your nutritional status, level of physical function and identify any dietary risk factors for surgery. Your diet will be assessed to determine whether changes are needed and nutritional supplement drinks will be recommended if necessary. You will be followed up by the dietitian until your transplant, and also after your transplant.
Dentist
All patients undergoing transplant assessment need a full check up with their dentist. The mouth can hold many bacteria and some of these bacteria can cause infections in the post-transplant period. Please ensure you speak to your doctor to organise antibiotic cover for any dental treatment. If you need teeth removed this may need to be done as an inpatient due to bleeding concerns. Please discuss with the liver transplant team.
Pastoral Care
Pastoral carers are available for the spiritual and religious care of patients and their families. Pastoral care is available during office hours and on call at other times for inpatients. If you would like to be visited by a member of your faith, please ask the staff to contact them for you. The Worship Centre is situated on the ground floor of building 1, opening hours 6.30am to 9pm daily.
Mental Health
Good mental health is incredibly important to our well-being, yet 20 per cent of the general population in Australia are affected by mental health issues in any one year. Poor mental health can show up in many ways. Some of these include low mood, depression, anxiety, sadness,
fear, loneliness, general unhappiness, lack of fulfillment, meaninglessness, insomnia, feelings of being out-of- control or of hopelessness, suicidal thoughts, phobias, schizophrenia, bipolar disorder, eating disorders and more. There is often a strong relationship between poor mental health, grief, and substance dependence. Unresolved mental health issues can contribute to housing, employment, relationship and other personal or social stress and crisis.
It is important that any past and present mental health concerns are identified. Patients often describe the huge relief in talking about and addressing their mental health, this sometimes being the first time they have done so. It is never too late or early to seek help for a mental health check. Compassionate and professional supports can be quickly put in place, achieving very helpful outcomes.
Occasionally, transplant recipients suffer significant psychiatric symptoms in the first few months after their operation such as depression, anxiety, mania, psychosis and body image issues.
The Liver Transplant team is supported by the Mental Health Service of the Princess Alexandra Hospital. Specialist mental health staff can provide assessment and treatment of mental health problems that may arise at any stage during the transplant process. Please discuss with your hepatologist or the liver transplant coordinator.
Until liver transplantation commenced in the 1980’s as a treatment for advanced liver disease, patients had a limited chance and faced certain death. Development of liver transplant programs offered new hope and enabled many adults and children with liver disease to experience the amazing benefits of transplantation, including a significant improvement in health, quality of life, and of the lifespan itself. Liver transplantation has been praised by many as a miracle.
A number of people with liver disease will either not have the opportunity for a transplant or will experience an unsuccessful transplant outcome. One of the issues is the shortage of donor organs available for transplant, compared with the number of people needing a liver transplant. When a donor liver does not become available in time for a patient, or when a re-transplant is not possible, or if a post-transplant patient develops another life threatening medical situation; the patient
will progress to the point where they might need palliative care. Palliative doctors and nurses provide supportive professional care when other treatments might not be so useful or possible. The palliative care team also supports the needs of patient’s carers and loved ones. The focus of palliative care is upon providing compassionate physical, emotional and spiritual care and comfort to the patient and their family.
How would I know that I need palliative care?
If transplantation is not a viable option or if a previous transplant is failing and re-transplantation is not possible, your doctor will discuss the different treatment options with you and your family. One possible outcome might be a referral to palliative care service.
How would I start palliative care?
If it is agreed that palliative care is a suitable treatment pathway for you, then you will be referred to the palliative care team. If you are an inpatient of the Princess Alexandra Hospital (PAH), the Metro South palliative care staff will explore the options with you and your family. If ongoing inpatient care is needed, you might be transferred to your local hospital and the palliative team for ongoing support. Or, you might stay as an inpatient of the PAH and your care would be managed by both the PAH hepatology and palliative care teams.
If you are an outpatient at the time, then you would be referred to your local palliative care service for ongoing support at home. There are palliative care services throughout Australia, including your general practitioner, specialist palliative care doctors, nurses, social workers, counsellors, psychologists and other health care specialists.
Where do I receive palliative care?
Palliative care can often be provided at home. Many people prefer to be cared for in familiar surroundings and where possible, this wish for home-based care is supported. Sometimes it becomes necessary to receive care in a local hospital or in a palliative care unit within a hospital setting, if your medical or nursing needs are too much to be provided at home. Home might not be the most suitable place for some patients and their families. Care can often be shared between an inpatient facility and the home, in order to provide respite for the family and optimal management of the patient. Flexibility and choice are the keys to good palliative care. Generally, palliative care is at no or low cost to the patient and family.
Can palliative care teams assist with pain management?
Pain management and easing of symptoms is a major role of palliative care. There are many ways in which pain and other symptoms, for example nausea, breathing problems can be helped. Your doctors will be able to explain your medication needs in more detail to help with your needs. Most palliative care services provide 24-hour phone support.
How else can palliative care help?
Counselling and pastoral care is available, and volunteers can provide a break for carers. Through the palliative care services, families and carers can connect with others in the same situation, many finding this network of support comforting.
The pharmacist works with your doctors and nurses to ensure you receive the correct medication. The pharmacist is available to discuss your medications with you. If you have any questions about your medications, just ask!
It is very important that you keep taking your medications, exactly as prescribed. If you forget to take your medicine, your symptoms will become worse. Please make sure you have enough medication to last until your next clinic visit and keep your repeat prescriptions in a safe place.
Do not take any other medications or supplements without asking your doctor or pharmacist first. Many medications, alternative therapies and supplements are toxic to the liver or may interact with your prescription medications. This includes medications bought from the pharmacy or supermarket, dietary supplements, for example vitamins and minerals and herbal or natural remedies.
Three of the most common medications used to treat the complications of liver disease are discussed below.
Propranolol (Inderal®, Deralin®)
Propranolol is a medication used to lower blood pressure and belongs to a group of drugs called beta-blockers. In liver disease the pressure in the blood vessels around the liver can be high. This is called portal hypertension and can lead to or worsen other complications of liver disease such as ascites and oesophageal varices, swollen veins in the oesophagus). Propranolol treats portal hypertension by reducing the pressure in these portal veins and varices.
Important information
When Propranolol is first started it may affect your mental alertness and coordination.
If affected, take care when driving or operating heavy machinery.
Possible side effects
Fainting or severe dizziness, slow or irregular heartbeat - seek medical advice
In liver disease excess fluid can build up in the abdomen and is called ascites. Diuretics are used to help remove this fluid and any fluid which may build up in the legs or lungs. Diuretics work by increasing the amount of salt and water you urinate and therefore increase the number of times you have to go to the toilet. Do not stop taking your diuretics without talking to your doctor.
Important information
Potassium is an important salt in the body.
Different diuretics can cause either a loss or gain of potassium.
Generally, frusemide and bumetanide cause a loss of potassium, while spironolactone and amiloride cause your body to retain potassium your doctor will be monitoring the potassium in your blood and will adjust your medication accordingly.
You may need to take potassium supplements if your potassium level is low.
It is very important that you talk to your doctor or pharmacist before taking any dietary supplements, for example vitamins or herbal preparations
You must also tell your doctor if you use salt substitutes as some of them contain potassium
Possible side effects
Skin rash, hives or itching - seek medical advice
Dizziness or light-headedness, rise slowly after lying down or sitting
Upset stomach or diarrhoea
Ringing in the ears with frusemide and bumetanide - seek medical advice
Breast tenderness in women with spironolactone only
Breast swelling and tenderness in men - spironolactone
Hepatic encephalopathy is a disorder of brain function that can result in drowsiness and confusion. It is thought to be caused by a build up of ammonia and other toxins in the body. Lactulose can prevent and reduce the symptoms of hepatic encephalopathy.
The dose of lactulose is normally 10 to 20mls, 2 to 3 times a day. The dose is adjusted to produce 2 to 3 soft bowel motions each day. Lactulose may be mixed with half a glass of water, milk or fruit juice to make it taste better.
If severe hepatic encephalopathy happens it may be necessary for you to have the lactulose as an enema.
If this confusion occurs at home, please seek medical advice quickly
Possible side effects
Severe diarrhoea, if this occurs contact your doctor
Bloated feeling
Flatulence or wind
Stomach cramps and pains
Nausea
It is important to have an informed discussion with your doctors and pharmacist before your transplant
You should keep a list of your medications, ‘DMR’ Discharge Medication Record with you and bring it to each appointment. The pharmacist can produce new medication lists should changes be made or you lose it.
Case discussion and assessment presentation
Once all the investigations have been completed and reviewed, doctors will discuss your treatment options. If suitable your case will be presented to the liver transplant assessment committee.
Determination of suitability for liver transplantation is complex and done on an individual basis, looking at all aspects of your health and psychosocial situation.
The committee includes physicians, surgeons and other health workers involved in this specialty. The meeting is held at the Princess Alexandra Hospital. The liver transplant recipient coordinator will provide you with the details a week or so before the date of presenting your case.
Will I make the list?
There are some reasons that transplant may not be recommended as the best treatment for you. Some common reasons include:
Severe heart or lung problems.
Cancer of another organ, for example breast or bowel cancer.
Liver cancer is too big, too many or it has spread into the blood vessels or outside of the liver.
Technical problems that would make the surgery itself very difficult and or complicated. Examples include presence of blood clots in the liver veins or arteries and some forms of previous abdominal surgery.
Lack of social supports.
Continued substance abuse, for example continuing to drink alcohol, use illicit drugs or smoking.
Advanced age.
Too unwell.
For some patients, liver transplantation may not be recommended by the liver transplant team. In this situation, you may return to the care of your referring doctor or a referral may be made to the palliative care team depending on your specific needs.
The liver transplant waiting list
Once medically accepted as a possible recipient, you will continue to be monitored by the liver transplant hepatology team in the outpatients or as an inpatient.
It is important to know that the transplant team will continue to monitor your medical condition during this waiting period. If your condition worsens, it may be necessary for you to come into hospital for extra care or come off the waiting list if your medical condition deteriorates severely. Not all candidates listed for a liver transplant live to receive a transplant.
Staying in Brisbane after the transplant you will need a support person. Due to the time frames involved in the transplant process you will need to live within 4 hours travelling distance by car from the hospital. You must have clear lines of communication with the hospital. If you live further away, it will be necessary for you and your family to move to Brisbane or near to Brisbane. The social worker will be able to assist you if moving is necessary.
The transplant coordinator will need to have more than 1 phone number, one being your personal mobile, in order to call you when a suitable donor liver becomes available.
The waiting process can be difficult and stressful, with many unknown factors. You may feel frustration due to the loss of freedom and being required to be contactable 24 hours a day and the seeming inactivity during this period.
You may even start to think that the transplant team has forgotten you. Please be reassured that you have not been forgotten. It is important to remember that no one can predict when a donor liver may become available. It could be days, weeks, months or even years. Waiting is a matter of attitude. You can wait passively for the transplant to make you better, or you can use the waiting time to get yourself into the best possible condition for one of the most important events of your life. Follow medical advice as prescribed, eat well and exercise regularly to keep your body healthy and well prepared.
Model for End stage Liver Disease (MELD)
MELD is used to prioritise and allocate adult patients waiting for a liver transplant. It is based on a statistical formula that predicts which individuals are most likely to die from their liver disease.
Patients waiting for liver transplantation need a donor with the same blood group as the recipient. It is also important to have a good size match between the donor liver and you, the recipient.
What is MELD and how will it be used?
MELD is a numerical scale, ranging from 6 which is less ill to 40 which is gravely ill. It gives each patient a ‘score’ or number based on how urgent he or she needs a liver transplant in the next 3 months. Research has shown that MELD accurately predicts most patient’s short-term risk of
death without a liver transplant. The MELD score is also used to identify patients who are too well and do not need a liver transplant.
The number is calculated by a formula using 3 routine laboratory test results:
Bilirubin, which measures how effectively the liver excretes bile.
INR, prothrombin time, which measures the liver’s ability to make blood clotting factors; and
Creatinine, which measures kidney function. Poor kidney function is often associated with severe liver disease.
The majority of patients waiting for a liver transplantation have chronic liver disease and are listed as Category 3 and have their MELD score calculated regularly. A patient’s MELD score may go up or down over time depending on the status of his or her liver disease. Your MELD score will be assessed monthly whilst you are on the waiting list. This will help ensure that livers go to the sickest patient, that is the person in greatest need at that time.
Category 1 and 2 patients have acute liver failure and a very short life expectancy without a transplant. These patients have the highest priority to receive an organ and are not affected by the MELD system.
Support Through Education Program (STEP)
The Liver Transplant Support Through Education Program (STEP) has been running since 1998. STEP’s purpose is to provide information and support to all patients and families, especially when waiting for a transplant and during the early post-transplant months. Details about STEP are provided directly to patients when listed for transplant.
The STEP booklet has informative, easy-to-follow sections providing access, information and support to all patients and their families from wherever they are.
Patients on the waiting list and families often comment that participating in STEP helps them cope before and after their transplant, and that the information and support is helpful and reassuring.
The Donor
Individuals with irreversible liver failure are offered hope through liver transplantation. A liver is matched between a donor and recipient based mainly on the MELD score of the recipient, the blood group and body size. When the transplant team are notified of a potential organ donation, the doctors discuss who will be the best match for the organ based on these things. The length of time that someone has been waiting does not factor in these decisions.
The donated liver will come from a person who has died in an Intensive Care Unit. The family of the donor will have authorised and consented to proceed with organ donation on behalf of their deceased relative.
Organ donation only ever occurs after a patient has died in an Intensive Care Unit in a hospital. Death can be declared by the neurological determination of death (when the brain has died) or after circulatory death (when the heart has stopped).
Before donation occurs, the donor is assessed medically and screened for transmissible disease.
Care for the donor and their family throughout this process is provided by the doctors and nurses in Intensive Care, social workers and the DonateLife donor coordinators who are specially trained intensive care nurses.
These donations are made possible only by the generosity of families during a difficult time for their family. You can show your respect for the donor and family by caring for your transplant liver for the rest of your life to the best of your ability.
What happens when you are notified that a donor liver is available?
When a suitable liver is offered, the hepatology consultant or transplant coordinator will call you. This may be any time of the day or night. The transplant may not happen for many hours after this phone call. You will be generally be asked to make your way to the hospital shortly after the call. You have time to pack a bag. It is important that you do not drive recklessly or speed as you make your way into the hospital.
If you arrive during office hours, you will be asked to come to the Admissions area on the ground floor. If it is after hours, you will come to the front desk of the Emergency Department. You will be directed to the Transplant Unit which is located on the 4th floor on Ward 4BT. If you are an inpatient, you will leave for theatre from Ward 4E.
When you are called, you will be told when to stop eating or drinking. For 6 hours before any operation it is important that you must not have anything to eat or drink. When you have an anaesthetic, all the muscles in your body relax. If you have food in your stomach, it can reflux back up into your mouth and even worse, your lungs. This can produce a life-threatening pneumonia. It is alright to take your normal medications with a sip of water any time before surgery. It is also fine to brush your teeth.
The nursing staff will prepare you for surgery. You will be weighed, and have your temperature, blood pressure and pulse checked. The nurse will ask you if there are any implants or metal in your body. We ask this because we need to place an earthing plate on your body during the surgery and need to keep it away from any internal metal.
You will have many tests just before the transplant, including a chest x-ray, ECG, blood work, an alcohol test, groin and nasal swabs. If you have cancer in your liver, you may have a CT scan to make sure the cancer has not gotten worse while you have been waiting for the liver transplant. You will meet one of the junior doctors from the transplant unit who will go through the surgery one more time and make sure you don’t have any current illnesses or infections that will make it risky to go ahead with the transplant.
You will be asked to shower and remove all your clothes and underwear. You will change into a theatre gown and paper underpants. You will be measured and fitted with white, knee high
stockings to prevent clots in the legs. In theatre you will have a pair of pneumatic leg massagers placed on your calves to keep the blood in your legs moving while you are asleep. This prevents clots in the legs. The look is complete with a puffy paper hat. It is a good idea to remove all your jewellery and give it to your support person for safekeeping. Your clothes, glasses and other items will be put into a bag and placed into a locker whilst you are in theatre. You will be reunited with them when you return to your room in the ward or intensive care.
Many people have bacteria living on their skin that have been given special names by hospitals. It is likely you will know this from a previous hospital admission. This does not mean you have an infection. We all have bacteria living in and on our bodies and some are resistant to certain
antibiotics. It is best if these bacteria are not passed onto other patients as it promotes antibiotic resistance. If you are MRSA “golden staph”, VRE, CRE or MRAB positive, then isolation precautions will be taken throughout your stay in the hospital.
If you have false teeth or plates, please leave them in. It makes it easier for the anaesthetist to help you breathe as you go off to sleep. If needed, the anaesthetist will remove them after you are asleep, and they will be returned to you when you wake up.
You will have an ID band placed on your wrist and ankle. You will then go through many repetitive identification checks to make sure we have the right patient and that everyone agrees on the operation you are having done. You will be put on a bed and then you will wait until it is time to go to the operating theatre. You may wait a long time. This may be quite stressful and you can get
hungry. Once we have received confirmation that the liver is suitable, you will have an intravenous line (IV) inserted and the first doses of anti-rejection medicines and antibiotics will be given.
It is important to understand that you can complete all this workup and be waiting to go to surgery only to be told that the transplant has been cancelled. These false starts may happen more than once and can be a real emotional rollercoaster. There are several common reasons for not going ahead with a liver transplant which are helpful for you to know. When a potential organ donor is being evaluated, we do many tests, but the final decision to go ahead with the donation cannot be made until our transplant surgeon has examined the liver. Only then, can we be confident that the liver is healthy and alright to use. Once our surgeon calls to say that the donor liver is acceptable, you will then be taken to the operating theatre, but your own liver is not removed until the ‘new’ liver has arrived at the hospital.
The operating theatre
When everything is ready to proceed, you will be wheeled around to the operating room by a theatre orderly and a nurse. This is where you will say goodbye to your relatives. At the end of the operation, the transplant surgeon will call them, letting them know how things have gone and when they can visit you.
The next stop is the anaesthetic room. This is a small room next to the main operating theatre. You will meet the nurse assisting the anaesthetist. You will then have another identification check, you will be very good at reciting your name by this point. The nurse will check that your consent form is completed.
There will be 2 anaesthetists looking after you and if they haven’t met you earlier, they will say hello and go through your medical history again.
You will already have an IV in, so there is nothing else that will go in your body while you are awake. You will then be taken into the main operating theatre. This can be a confronting place. There may be several people in the room, all wearing masks, talking and preparing the theatre. They are all there to look after you.
Most operating theatres are set up in a certain way. There will be an anaesthetic machine with lots of the monitors to keep an eye on you. There will be tables filled with surgical instruments, ready to perform your transplant. There will also be nurses preparing this equipment and counting each and every instrument to ensure that we have everything we need. There may also be junior
medical staff and orderlies. The operating table is in the middle of the room beneath the big lights. They will not be turned on until you are asleep. The operating table is narrow and cold. It is narrow because we need to stand close to you to operate and it won’t be cold for long because during the surgery you will covered with a heating blanket.
The trolley you are on will be placed beside the operating table and if you are mobile, you will be asked to move yourself across and onto it. If you are in pain or not mobile, we will slide you across to the operating table on a special board or float you over on a noisy hover mattress. A lot of activity will then happen around you. We will place padded boards on the side of the bed for you to rest your arms on. Your leg massagers will be hooked up and switched on and you will feel gentle compression on your calves.
You will have 3 stickers placed on your forehead. This helps the anaesthetist monitor how deeply asleep you are. Sticky dots to monitor your heart beat will be placed on your chest. Fluid will be hooked up to your IV line and a clip that reads your pulse placed on your finger. A blood pressure cuff will be wrapped around your arm and the first time it takes your blood pressure, it will inflate very tightly. It will only do that once.
You may already be feeling happy, drowsy or talkative as the anaesthetist may have given you a relaxing medication via the IV. You will not go to sleep yet, but it is unlikely you will remember anything after this until you wake up in intensive care.
The Anaesthetic
Sometimes knowing what happens during an anaesthetic really helps you relax and realize that you are well taken care of while you are asleep. Many people’s greatest fear is the anaesthetic. They worry about vomiting afterward, being aware during surgery and not waking up. Whilst these things very rarely occur, having an anaesthetic is actually far safer than anything you have already done that day, like driving into the hospital.
Once you are asleep, the anaesthetic team will work on your for about 2 hours before the transplant operation can begin.
General anaesthetic consists of 3 phases
1. Going to sleep – similar to taking off in a plane.
Just before you go to sleep, the anaesthetic nurse will ask you to breathe into a mask and fill your lungs with oxygen. This makes sure that you have the maximal amount of oxygen in your blood.
This does not put you to sleep. A white medication called Propofol is then given through your IV. The anaesthetist will ask you to keep your eyes open. As this medication goes into your veins, it can cause a stinging sensation in your arm. This is normal and does not damage you. After this injection you will be asleep in about 10 seconds. Your breathing will temporarily stop and the anaesthetist will take over your breathing for you by blowing oxygen into your lungs. As soon as you are asleep the anaesthetist will give a medication that stops your muscles moving. This has many functions. It allows your throat to relax so the anaesthetist safely place the breathing tube into the windpipe. It also relaxes your abdominal muscles and makes surgery on the abdomen easier. If you have false teeth, they will be removed at this point and returned to you in recovery.
As soon as the muscle relaxer has worked, the anaesthetist will use a special tool called a laryngoscope. This is a smooth spatula with a light that is inserted over your tongue and deep into your throat. The anaesthetist will be able to see your vocal cords and beyond this is your trachea or windpipe. A specially designed hollow tube is placed down the spatula and into the windpipe. A balloon on the end of the tube is inflated by the nurse to fully occlude your airway and stop any vomit or secretions from entering your windpipe.
This is often the trickiest part of the anaesthetic and your life can depend on it. There are many signs the anaesthetist will look for before you go to sleep to predict whether getting this tube down will be difficult or not. If you have a small jaw, previous difficulties with intubation, neck problems, difficulty opening your mouth, the anaesthetist will be ready with a different strategy to get the tube down your throat safely. Because your breathing is our number one priority, occasionally putting the breathing tube down can result in damage to your teeth or cuts to your lips. All care is taken and this is uncommon. Having a tube in your throat can leave it sore and dry for a day or too. This is temporary. You have also have a swollen uvula, the dangly bit at the back of your throat for a few days.
Before the surgery starts, you will be given a dose of antibiotics via your drip to help lessen the risk of wound infection. Soft tape will be placed over your eyes to keep them closed and protected. Your arms and legs will be padded to protect your pressure areas and you will be positioned for surgery.
You will have many tubes placed into the blood vessels of the neck and groin and wrist. You will have a catheter put in your bladder.
There are other devices we use to monitor your wellbeing during surgery.
2. Staying asleep during the surgery – cruise control
You will be kept asleep by anaesthetic gas piped in via the tube in your windpipe or by a continuous infusion of Propofol in your drip. The anaesthetic machine will steadily and precisely breathe for you. Your anaesthetist will never leave your side and constantly monitors your vital signs. They will give you small doses of medications and fluids to keep everything steady. It is very common that you will need a blood transfusion during transplant surgery. Any blood that you lose during the operation is washed and processed by a special team and returned to you via your IV.
3. The end of the operation
As the surgery comes to an end, the anaesthetist will prepare to take you around to intensive care. Frequently they will continue your anaesthetic and you will stay asleep. Once your condition has stabilised you will be woken up in the intensive care. This may be in a few hours. In some circumstances, if you are very unwell, you may be asleep for many days. You will not remember this.
The liver transplant operation
Liver transplantation is considered to be the most difficult of all transplants. The surgery takes between 4 and 12 hours.
It happens in two parts
The removal of your liver, a Hepatectomy or Explant
Sewing in the donor liver, the transplant
Step 1: Removing your liver
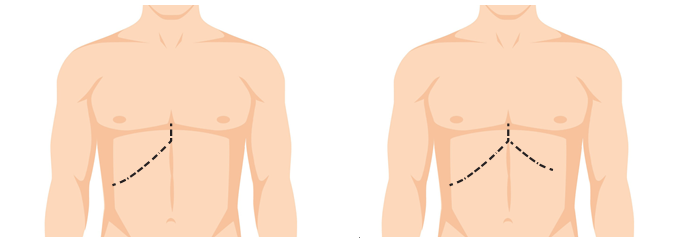
The operation will begin with the surgeon making a large cut on your upper abdomen. This might be on the right side – called a Hockey Stick or cover both sides of your belly – called a Mercedes Benz incision. See Figure 1
Figure 1. The types of wounds we make to do a transplant. It may be on one side, a Hockey Stick or both, a Mercedes Benz.
If you have a lot of fluid, or ascites, in your tummy, it will all be removed by suckers. This fluid may accumulate again after the transplant. Because the liver is high up under the ribs on the right side, an elaborate metal frame, or a retractor, is used to pull the ribs up so the team can work.
When everything is set up and the view is optimal, the next task is to cut out your failing liver. This is all about setting up your blood vessels to join the new liver to them. Getting the old liver out can be the most demanding part of the operation. The massive varicose veins that surround the liver and coat every surface of the abdomen can bleed with the slightest touch. Because the old liver does not make clot well, this is the phase of the operation where the most blood can be lost.
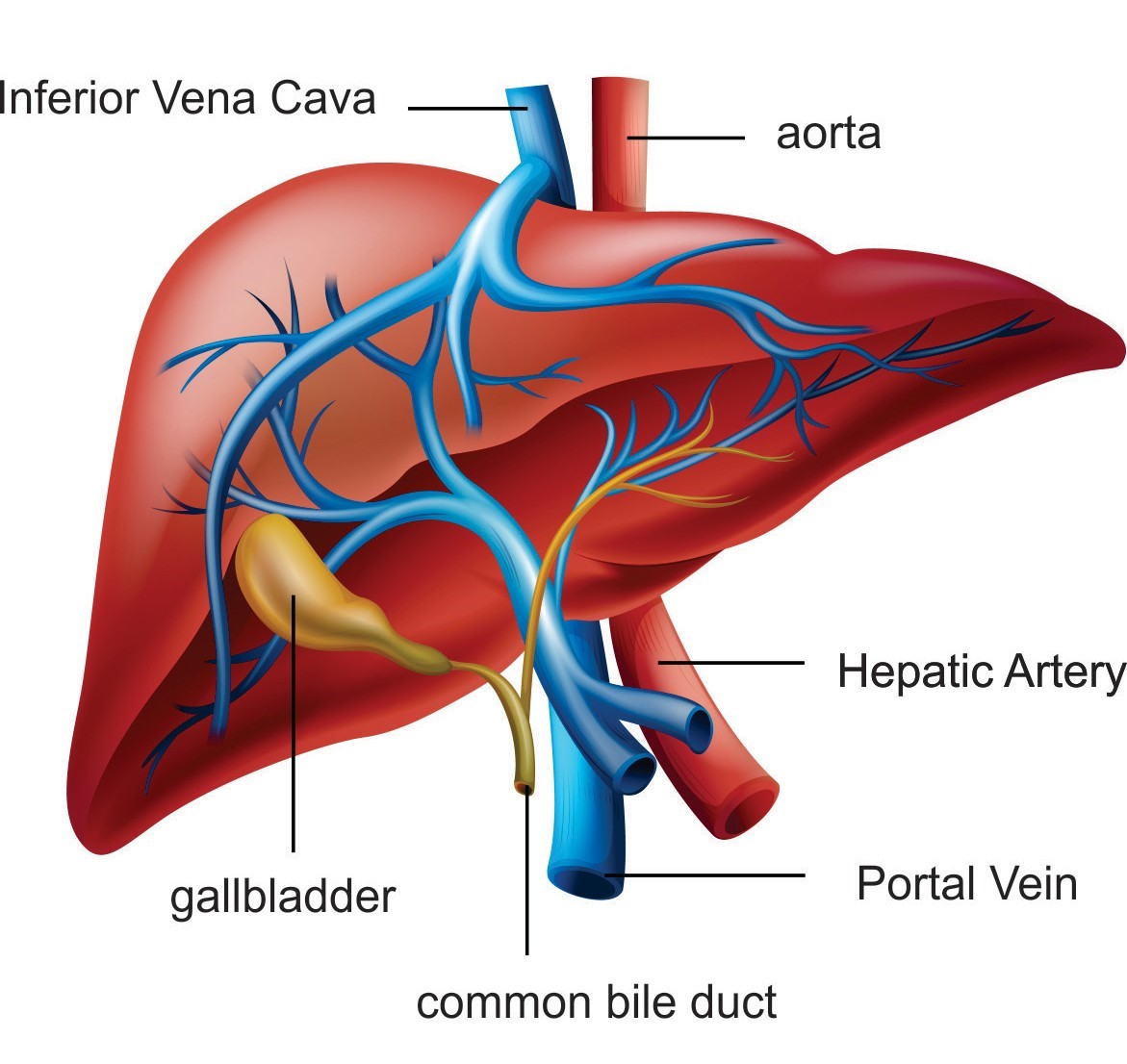
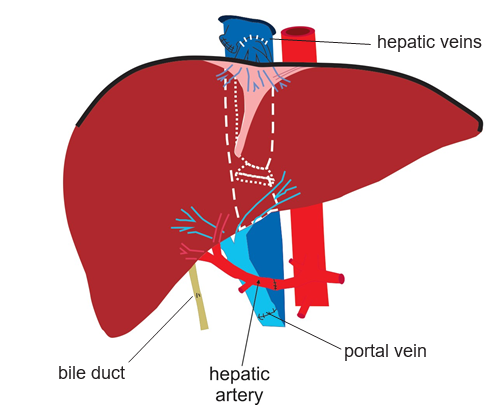
The liver must be freed from all its attachments. To understand this better, a quick lesson in liver anatomy is needed. For such a big organ, about 1 and a half kg, depending on the size of the person, the liver has very little in the way of attachments to the body. Aside from a few flimsy ligaments, the only things that really hold it in place are its blood vessels. The liver is unique because it has two separate blood supplies. Figure 2
The first is the hepatic artery that brings blood with oxygen, straight from the lungs via the heart. The bile ducts are the main beneficiary of this blood and it is for this reason that the hepatic artery is the Achilles heel of liver transplantation. If the blood stops flowing in the hepatic artery at any point after the surgery, very few livers will survive. The fragile bile ducts will die and liquefy forming lakes of bile within the liver. These pools will become infected and it is likely that you will need to be re-transplanted. This can happen at any time in your life but the risk is highest in the first few weeks after transplant.
The second blood supply to the liver is the impressive but delicate portal vein. The size of a garden hose, the portal vein drains blood from the bowels, stomach and spleen. It gives the liver cells the first pickings of the nutrients, fats and toxins produced by the gut. But the only things that really hold the liver in place are the imposing hepatic veins. Like everything in surgery, what goes in must come out and the hepatic veins are how the blood flows out of the liver. These are the 3 stout tributaries that return the blood from the liver almost directly into the heart. These hepatic veins are the most significant support structures for the liver and incredibly, only a single row of tiny stitches between these veins are all that is required to keep the new liver in place.
Figure 2. The blood vessels and bile ducts of the liver
The Back Table
While the surgeon is working to remove your liver, another surgeon is preparing the donor liver in a process called “The Back Table”. This is where the unnecessary tissue is stripped off the blood vessels going to the liver in order to gain as much length as possible. The liver is kept in a bath of ice-cold solution while this is done.
Step 2: Sewing in the donor liver
When everything is ready, the blood vessels in and out of the liver are clamped and your old liver is removed. We must work very quickly to sew the new liver in so your blood can start flowing through it. The liver is “Piggybacked” onto the blood vessel that brings blood back from your lower body to your heart. This takes about 30 minutes. See Figure 3
Figure 3. The “Piggy Back” technique for sewing the new liver in
The new liver is taken out of the cooler and brought onto the operating table. Ice cold salty water is hooked up to a tube in the portal vein of the new liver and poured through at full speed to keep the liver cool and to flush out all the preservation fluid.
The first join up, or anastomosis, is the hepatic veins. The portal vein is next. This will bring most of the blood into the liver. It is relatively easy to twist this vein or make it too long, so a great deal of judgment must be used to cut it to just the right length. When these two join ups are complete, it is time to release the clamps and let blood into the new liver.
The cold liver once again becomes warm as the blood rushes in and returns it to its familiar rich, red colour. The liver will swell, becoming about 30 per cent bigger, expanding to fill the space where the old one used to be. This is the point where you hope the size match between the donor and recipient has been estimated correctly. If the liver is too big, it will bulge out of the abdomen making it very difficult to look for bleeding behind the liver. If it is too small, it may not be enough to function.
In the moments after blood rushes through the new liver, it is a very dangerous time. Your blood pressure may become unstable as the toxins that have built up in the bowels are released into the circulation and there is a second wave of bleeding. This is the time during the transplant that you are at highest risk of dying. The new liver takes some time to start working and the blood, still affected by the ravages of cirrhosis will take a while to clot. Little holes in all the blood vessels begin to open up one after another with the changes in pressure and each one needs to be attended to with fast precise stitches.
Once the bleeding has settled down, attention turns to the hepatic artery. Now, the pace of the operation slows down a lot. Joining this artery together is a painstaking job that must be
performed with technical perfection. About this time the liver will be starting to work a little. Clots are produced and slowly the bleeding will ease.
The final step in the operation is to remove the donor gallbladder and then join up the bile duct. Most livers will start to produce bile straight away.
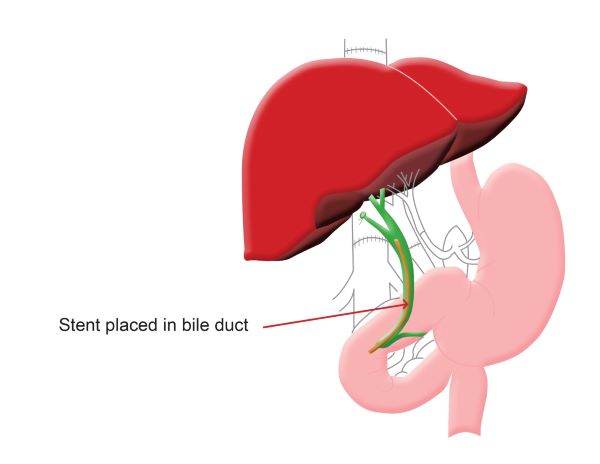
There are 2 ways to hook up the bile duct
Duct to duct (Figure 4): Your bile duct is joined directly to the donor bile duct. Sometimes a piece of plastic tubing or a stent is placed inside your bile duct during this process. 80 per cent of patients will pass this stent into the toilet with their bowel motion and the other 20 per cent will need it removed after the transplant. This is done via an endoscopy.
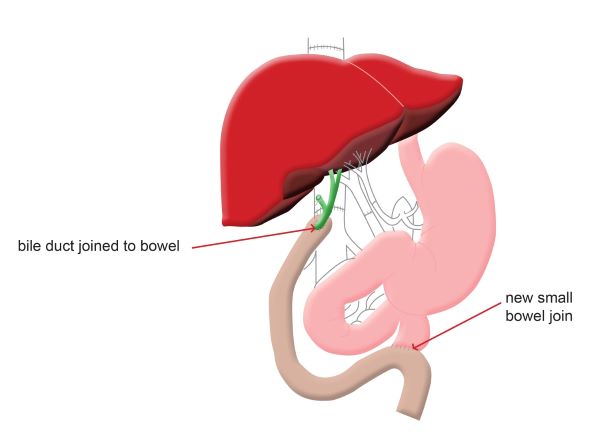
Roux-en-Y, pronounced Roo-on-why (Figure 5): This is done for patients with diseases of their bile ducts or when there is a large difference between the size of your bile duct and the donor. The donor bile duct is sewn onto a section of your small bowel.
Figure 4. Duct to duct (Internal Stent) Figure 5. Roux-en-Y
After completion of the bile duct connection, several large drain tubes are placed around the liver to drain away the fluid and blood. The abdominal wall and skin are closed and you will be moved to the intensive care unit.
Variations in the liver transplant operation
“Split” Liver Transplantation
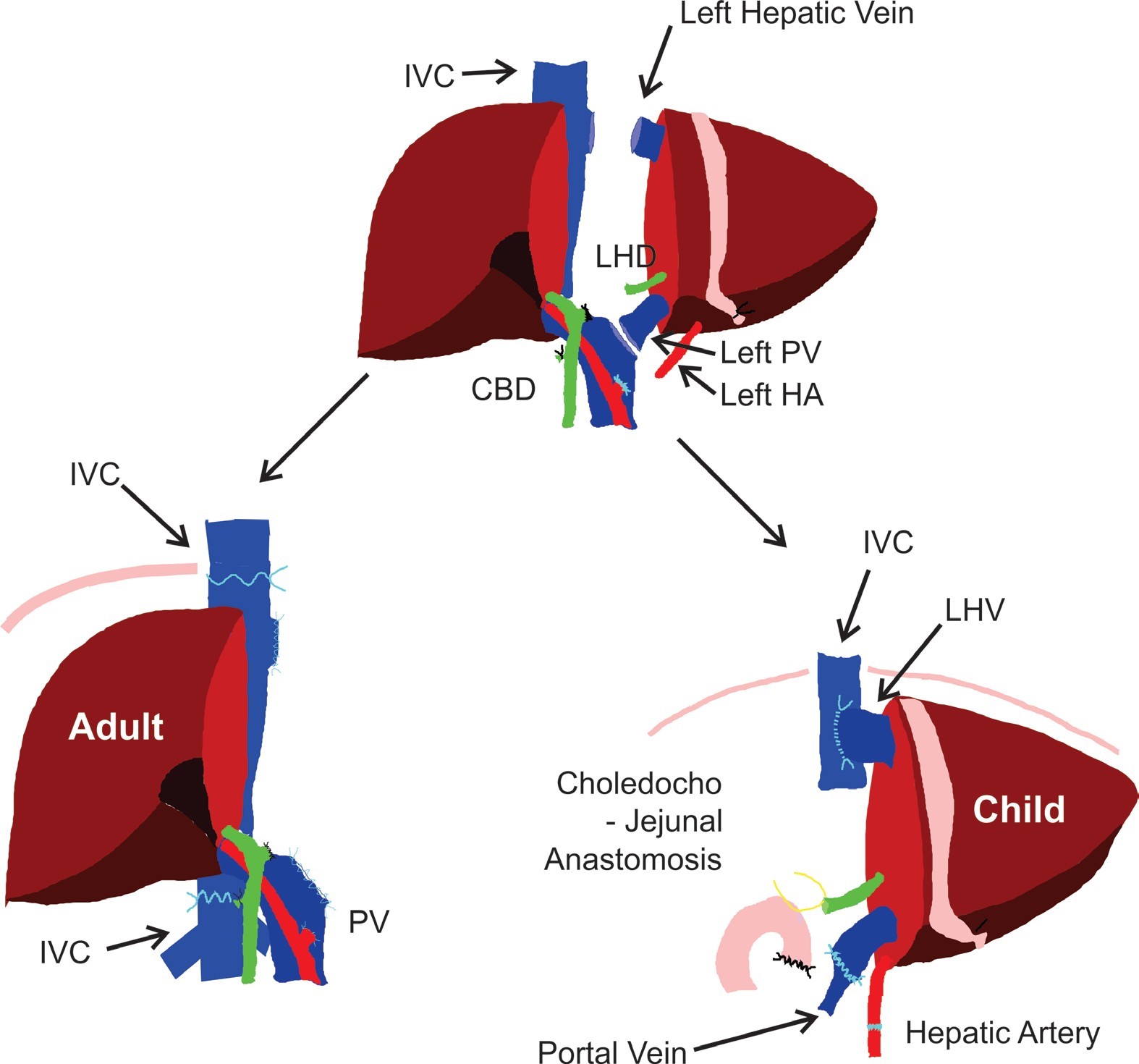
Many patients will receive a whole donor liver. Because children having a transplant need a very small piece of liver, we will sometimes split a liver in half. The left side will be given to a child and we will use the right side for an adult. This is a good way to make the most out of a very precious thing. This is called Split liver transplant. Figure 6
This technique was developed in Brisbane and is now used around the world. The liver tissue, blood vessels and bile ducts need to be divided, increasing the possibility of bleeding and bile duct problems after surgery.
Figure 6. “Split” Liver Transplantation
Organox
The Queensland liver transplant service will sometimes place the donor liver on a machine called Organox before transplant. This machine passes blood and nutrients through the liver. For many reasons, there are some donor livers that may not work well. This can be very difficult to figure out.
This machine will tell us with some certainty, whether the liver will function well after transplant. If the liver works well on this machine, it is likely to work well in you. You will be told if we are going to use this machine for your liver. This machine lets us use many livers that may have not been used in the past.
Intensive Care Unit (ICU) patient information
You will be transferred to the Intensive Care Unit (ICU) immediately after your operation and probably before you wake up from the anaesthetic. You will have a registered nurse with you at all times.
This information is intended to help you and your family to become familiar with the machines and surroundings of the ICU. We hope this will help to address some of the concerns you may have regarding your time in Intensive Care. If you or your family have any questions do not hesitate to ask any of the staff.
Breathing
You will have a breathing tube, an E.T. tube, in your mouth and this is attached to a ventilator to help with your breathing until you are more awake. The tube lies between your vocal cords so you will be unable to talk when it is there. You will be well sedated while this tube is in, but it may be a little uncomfortable as you are waking up. When you are fully awake and breathing for yourself the tube will be removed. You may have a sore throat and your voice may be husky.
A physiotherapist will visit you several times during your stay. They will help you to take deep breaths and cough up any secretions from your lungs. You will feel some shaking and vibrations on your chest to loosen the secretions. While the breathing tube is in place we will remove secretions by passing a smaller tube down it and applying suction. This will cause you to cough and take your breath away for a few seconds
Tests
When you get to ICU you will have a chest x-ray, blood tests and an ECG, a heart tracing. These tests will be repeated daily while you are in ICU.
Pain relief
The nursing and medical staff will frequently check to see if you have any pain. Please tell us if you are sore or have any pain so we can attempt to relieve it. A pain score of 0 to 10 is used, with 0 being no pain and 10 being severe pain. It is important that you are relatively pain free and can cough and take deep breaths as this helps to avoid post-operative complications such as pneumonia. Pain relief is normally given through a Patient Controlled Analgesic machine with a push button that you will operate yourself. You will then be transitioned to pain relieving tablets. Overall, those who have undergone liver transplantation say that there was not as much pain involved as they anticipated. We believe this is due, in part, to the type of incision that is made, plus the use of steroid medications.
Noise
Intensive Care is a busy ward and can get quite noisy. While you are lying in the ICU bed without anything to do, noises will seem to be much louder than they actually are. Most of the noise is from monitor and ventilator alarms. Don’t be concerned if your monitor alarm sounds. Staff will explain what the alarms mean. We aim to have a quiet time from 10.30pm to 6am to let patients sleep, however, due to the needs of our sicker patients this cannot always be achieved.
The recovery period
Immediately post-transplant
After you wake up, you will have a lot of tubes coming out of your body. Most of these will be removed in the first week. The most uncomfortable one may be a nasogastric tube, a NG tube, in your nose. This helps to keep your stomach empty. It will usually come out on the first day.
You will be allowed small amounts of ice chips in order to keep your mouth from feeling too dry and it is likely you will be able to drink on the first day and eat within 2 to 3 days of the transplant.
You will have a Central Venous Line (CVL), which is a large intravenous drip, coming out of your neck. It will be needed to give you fluids and medications until you are able to drink and eat again. This line may be changed for a smaller one on the first day and then it will stay in for about 5 days. If your veins are bad, you may have a drip called a PICC inserted into your arm. This line can stay in for several weeks if you need it.
In order to empty your bladder and monitor your fluids, you will have a catheter in your bladder that will drain urine into a bag. The catheter is usually removed as soon as you are able to get out of bed. Your bowels will not move for 5 or 6 days after the transplant.
2 or 3 drains will come out of your abdomen and will be connected to plastic suction bottles. The drains will drain off any excess blood or fluid from around the wound that is common after a transplant. These drains will gradually be removed between the 2nd and 7th day after your surgery.
Tests
On the first day you will have:
a chest X-ray
an Ultrasound of the liver to check the blood vessels
frequent blood tests
After this, you will have daily blood tests and another ultrasound may be done if your liver tests rise. You may also need a liver biopsy to look for rejection.
The hospital stay
The average length of stay in the ICU is variable and largely dependent on your body’s tolerance of the surgical procedure as well as your pre-operative medical condition. Once you are stable, you will be transferred to 4BT, which is the Kidney and Liver Transplant Unit on the 4th floor Main building. You should expect to spend at least 7 to 14 days in the hospital post transplantation. If you experience complications it can be a lot longer than this.
After your transfer to the transplant ward, you will be seen by a physiotherapist who will instruct you on getting in and out of bed and work with you in rebuilding your strength.
You will also be encouraged to do coughing and deep breathing exercises in order to keep your lungs clear and expanded. This will help prevent chest infections. Remember that the location of your liver is in the right upper portion of your abdomen and is therefore directly below your right lung. This part of the lung can collapse during the surgery and fluid may collect in the chest cavity, called a pleural effusion. Frequent coughing and deep breathing will help this fluid get better and expand your lungs.
You will begin to eat shortly after transplant. You will begin with liquids and progress to solid food. Well-balanced, high protein meals are necessary because your body will need adequate calories and protein in order to heal and rebuild itself. Few dietary restrictions are necessary. To help with your individual needs, the transplant dietician will discuss and instruct you on foods that will be beneficial in this rebuilding process. Before discharge, the transplant dietician will counsel you individually on the long-term nutritional guidelines that you will need to follow.
Throughout your stay in the hospital, the transplant team will record your daily lab and test results on a computer. This will provide an overall picture of how you are doing. We feel that discussing your results and the intended plan of care while in your room provides an additional learning opportunity for you. Please do not hesitate to ask questions during this time.
Pharmacy—medications after your transplant
You will have the opportunity to attend an information session on the medications that you will need to take after you have received your transplant. It is very important you attend 1 of these sessions, as they will help you understand the importance of medications post-transplant.
Some important points to remember about medications after your transplant:
Following your liver transplant, you will take a lot of new medicines. These are vital to the success of the transplant.
It is important you never run out of these medications and do not stop them without being advised to do so by your doctors. Stopping these medications can lead to your transplant failing.
You will need to pay the PBS prices for these medications. Your pharmacist can provide more information and advice around costs and access to medication as you need it.
Before starting any supplements or herbal medications you must check with your doctors whether these are safe. Many supplements and herbal medications can damage your liver, lead to failure of your new liver and cause many side effects.
It is important to have an informed discussion with your doctors and pharmacist after your transplant
You should keep a list of your medications, ‘DMR’ Discharge Medication Record with you and bring it to each appointment. The pharmacist can produce new medication lists should changes be made or you lose it.
Rejection
The body’s normal response to anything foreign is to defend itself. In the case of an infection due to a foreign virus, fungus, or bacteria, this protective response helps us avoid getting ill. However, in the transplantation of organs, this normal function of the body called rejection is what we seek to prevent. We do this by giving immunosuppressive, or anti-rejection medications.
The primary anti- rejection medications used are Tacrolimus, Prednisolone, Azathioprine, Mycophenolate and Cyclosporin. These are used in combination according to your needs. There are many other immunosuppressive medications that may be used in addition to these.
Every individual needs differing doses of immunosuppression. Some need a lot, some need very little. There is no way to predict this. In spite of all the medications you will receive to prevent rejection, episodes of rejection can still occur.
Rejection occurs most frequently in the first 3 months after transplantation, when we are trying to find the correct level of immunosuppression for you as an individual. These rejection “episodes” are treatable and 9 out of 10 times are reversed with high doses of prednisone. There are other drugs we try if prednisolone does not work. Rejection episodes are part of liver transplant, we are prepared to diagnose and treat the rejection episodes accordingly.
The most common reason that people experience rejection after they leave hospital is that for one reason or another they forget or stop taking their immunosuppression medication. Missing even 1 dose can cause problems and you need to be vigilant about taking your medications every day.
There are very few symptoms when you are experiencing rejection. While in the hospital, and as an outpatient a rejection episode will most likely be recognized by an increase in your liver enzymes and bilirubin levels, on a blood test.
Less common symptoms of rejection may be:
Fever, a body temperature over 38 degrees Celsius
Yellowing of the eyes or skin
A general feeling of unwellness and fatigue.
When we notice a rise in your liver function tests, you will be sent to have an ultrasound to make sure all is well with the blood vessels of the liver. If we are concerned about rejection, a liver biopsy may need to be done. This small sample of tissue will then be reviewed under a microscope. Treatment for rejection will be commenced when we have the biopsy results.
It is important to take your medication as prescribed to help prevent rejection and call us if you are not feeling well
Donor family correspondence and information
Writing to your donor’s family
Receiving a card or letter of thanks is very special to the family of an organ and tissue donor. It provides the family with the knowledge that the donation has made a difference and helped others. Recipients often appreciate being able to say “thank you” in a letter or card.
This correspondence is anonymous, therefore it is important that you do not include your name and address or the hospital where you had your transplant. There is no right or wrong time to write to your donor’s family. It is when you feel ready. Information and brochures are available to assist with writing.
When you have written, place your card or letter into an unsealed envelope
On a separate piece of paper, provide your name and the date you were transplanted
Then send both of these to the DonateLife office at the address below:
Donor Coordinators DonateLife Queensland Building 1, level 4 Princess Alexandra Hospital Ipswich Road, Woolloongabba, Qld 4102
You may also make enquiries of the clinical nurse in the Outpatient department regarding any of the above information.
Duration 12:16|Closed captions icon
As a transplant recipient you may like to write a letter or card to your donor's family to thank them or acknowledge their life-changing or life-saving gift.
This video aims to provide you, as a transplant recipient, with more information about how to do this and to recognize the feelings and emotions that can be experienced by recipients during this time.
It is important to know that there is no time limit for writing to your donors family.
You can write when you feel ready which may be shortly after your surgery or many years later.
Only you will know when the time is right for you.
Many transplant recipients have said they struggle in writing to their donors family so please know you're not alone if you experience this.
Your transplant coordinator can assist you if you're having trouble and more information about what to include will be covered later in this video.
Most donor families love to hear from their loved ones recipients.
Receiving a card or a note of thanks can provide them with a sense of comfort knowing that the donation has helped others and that their gift was truly appreciated.
My mom was ... She was beautiful and I know we all say that about our mums but we had a closeness that a lot of people just said I've never seen a mother and daughter as close as you two are.
And that mainly came because my dad was killed in a car accident when I was two and so we did everything together.
She had beautiful blonde hair that's sat sort of just above her shoulders she had the biggest Bluest Eyes and she was just a wonderful, caring, compassionate human being.
Mum died in March probably nine months after... I wasn't in a very good place because I just turned 40.
It was my first birthday without her and I had amazing support around me but I really struggled, really, really, struggled with that. My heart was just broken.
The most profound letter that I received was from her lung recipient.
Her lung recipient said to me, my children are eternally grateful that I'm here to love and protect them.
In that moment, it was just like mum going get your backside off that ground to pick yourself up.
It was just this massive heartwarming sensation of my children were struggling they'd lost their grandmother not their mummy and their daddy.
It was this sense of calm and peace that came over. It was like everything is the way it's meant to be.
If a donor family does not feel ready to receive a letter or card, they may ask the Donate Life agency to hold on to it for them or families can place it somewhere safe to be opened in the future.
To provide them with that option your letter is placed in a separate envelope so they can read the cover letter from Donate Life and then decide when to open the second envelope.
This may be when the whole family is at home that day or a special time for the family.
Australia's organ and tissue donation program is confidential.
There are laws and policies in every state and territory that make it illegal for health professionals and Donate Life staff to share information that might publicly identify a donor or transplant recipient.
For this reason correspondence between recipients and donor families needs to remain anonymous.
It's important that you don't include details like your name or address, the name of your transplant doctor or the hospital where you had your transplant or any other potentially identifiable information when you write to your donor family.
It can be the hardest letter to write and on top of that it can feel a little bit unnatural because you're not writing to anybody you know and you're unable to put in the identifying characteristics really and about yourself either.
So we ensure that patients are educated on the process recipients can write.
I'm going to be able to see my three beautiful children grow up I've got this dream of owning my own shop and I'm going to be able to hopefully fulfill that dream.
If they've got any questions about how to start the letter or can you read a draft for me or you know is this appropriate we'll support them throughout the process if needed.
To begin your letter of card you may like to start with the doner family or make it more personal by saying dear friend.
Use Simple language.
Doner families like to know how you're doing, why you needed a transfer, how your life has changed since the transplant and about your family interests, hobbies or job.
Donor families also appreciate a simple thank you.
Two words can mean so much.
The length of your letter and the information you include is up to you.
We recommend taking a less is more approach.
Often simple thoughts and expressions of gratitude mean the most when sending your letter or card.
Consider signing off with a phrase such as from a grateful recipient or similar words that reflect your feelings.
Please don't send gifs or photos as these can't be passed onto your donor family.
Your heartfelt words will mean a lot.
If there are any aspects of the letter that your transplant coordinator is concerned about, they will discuss these with you.
Some people find it easy to write for others.
Writing may take time or even several attempts.
If you're finding it hard, your transplant coordinator can help you during the process.
It can be a very emotional and challenging experience and support is available.
There are also correspondence guidelines to help you with your correspondence.
These guidelines are provided to you by your transplant coordinator and can be provided again whenever you need them.
They are also available on the Donate Life website.
Writing the actual letter was something that I was very very keen to do and it's funny, uh, I'm a writer words come fairly easily to me when I'm sitting down in a blank piece of paper but that was the scariest blank piece of paper I've ever seen.
I struggled because I've never saved my life they've given me a chance to wake up on another Christmas morning with my son so how do you thank someone, you know, for that.
And it's simple like I just said thank you, totally overwhelmed. It was a ... it was a daunting task but the the short answer to that is you just say thank you.
It was cathartic and wonderful and heartbreaking and all the things you can imagine. It was part of my recovery and healing process, it really was.
As hard as it was to write um, it was it was an incredible experience writing it.
When I got the call when I got into hospital and I was and I got to give my sister a hug and her husband and and Henry, my son, we're very well aware of what was happening somewhere else and this, this is the dichotomy that I was
still never fully grasp that. At the same time that we are celebrating this chance at life somewhere there's a family that are suffering the deepest darkest day of their lives and in that grief somehow they've made the decision to save my life.
And they don't know me it's it's a, it's a lot to take on. Um, it's something that you never forget.
I understand how hard it is to write, I really do and and to try and find the right words and you're conscious of how are these words going to be taken.
People are quite concerned that they're going to upset, upset the donor family.
I'm with them about the family have gone through their Darkest Day already they have felt this sorrow and sadness but they gave their loved ones organs to help save someone else so they actually want to be validated.
They want to get your correspondence to say that you are doing so well and that you are now living your best life.
Every time I get a letter I do come undone I do get upset but it it allows me to grieve in a way I had a deep love for mum and Grace is the last gift that we have around that.
It allows us to process it too so when you actually get that letter the next day, you go back to it and the next day and the next day.
My advice to other transplant recipients that are perhaps struggling with where to start is just start with a thank you. So if you're not ready to write it straight away like I was, sit back wait wait a month wait a couple of months.
Wait six months it doesn't matter, but I promise you once you do it, as hard as it is to write, it you will feel better and I absolutely promise you that.
You don't... a family will feel better about it as well.
Someone gives me a cup of coffee, I say thank you. Someone gives me a chance of seeing my son wake up another day, you know that deserves a lot of recognition and gratitude.
I would say to the recipients when they're writing a letter, just speak from the heart. Tell us how you are, tell us how you feel, tell us what you've achieved what's going on in your world and what matters to you the most.
I feel like her recipients have given me the gift of healing.
As much as mum had given the gift to her in that moment, she reciprocated that gift to me through a letter.
When you've written your literal card, you can post or email it to your transplant unit or you can bring it to a follow-up appointment with your transplant coordinator.
To help maintain confidentiality, staff and the transplant unit will open and check your letter or card for identifying information before it is sent on.
If what you write includes any identifying information your transplant coordinator will get in touch to talk about and help you with any changes that may be required.
In some cases correspondence won't be sent.
This may be because it contains information that could publicly identify yourself, the recipient.
In other cases it may be because the donor family doesn't want to receive correspondence at this point in time. In this case it will be kept in the donor file ready to forward should the donor family change their mind about receiving correspondence.
It is important to understand there is no obligation for the donor family or transplant recipient to write or respond.
There's also no expectation for any ongoing exchange of correspondence.
Everyone has a different way of coping with the loss of someone they love.
If you don't receive a reply it may be that writing to you is very difficult for the donor family.
Donor families also receive ongoing support from their local Donate Life agency and are supported writing correspondence if they wish.
Some donor families say that writing about their loved one and the decision to donate has helped them grieve.
Some donor family members say they are very happy to have made the decision to donate and wish the recipient well, but don't wish to continue any correspondence.
Writing to your donor's family can be a positive experience for both you and the donor family.
Writing to your donor family is a personal choice and your transplant coordinator can support you and your decision.
Find out more about writing to your donor family. Talk to your transplant coordinator or visit donatelife.gov.au for more information.
Glossary
Angiogram (Arteriogram)
Under radiology conditions, dye is injected into the blood vessels in order to determine if there are any blockages in the arteries.
Arterial blood gas (ABG)
A small needle takes blood from your wrist to measure the level of oxygen in your arterial blood. This can be a painful test.
Blood tests
A large number of blood tests are needed pre-transplant to monitor your liver function and check for other diseases. We also test for blood borne viruses,
for example, HIV, hepatitis B & C, blood group, tissue typing, to match your new liver, and cholesterol levels. Some of these special tests need to be repeated whilst you are on the waiting list.
Bone mineral density
This examination establishes a baseline of your bone density, assessing the strength of your bones. Thin bones, or osteoporosis is a common complication of liver disease and can be made worse by some of the drugs for example prednisolone that will be given to you after the liver transplant.
Bone scan
This scan is requested if you have a history of primary liver cancer and looks for spread of the cancer to your bones. An isotope will be injected 2 to 3 hours before the procedure. The scan takes about 40 minutes.
Chest X-ray
The chest x-ray is taken as a baseline image of your heart and lungs. You will have yearly chest x-rays whilst you are on the liver transplant waiting list.
Colonoscopy
This procedure allows the doctor to look at the inside of your large bowel or colon. This test is important to check for polyps and exclude bowel cancer. Polyps will be removed and biopsies may be collected.
Preparation – you will be told to follow a clear fluid diet 24hours before the procedure, and a special bowel preparation is drunk to ensure complete cleaning of the bowel. A sedative is given before the procedure. The colonoscope, a flexible tube with a miniature camera, is passed into the bottom then gently guided around the colon. The procedure takes about 40 minutes.
Cardiopulmonary exercise test (CPET)
The cardiopulmonary exercise test measures the response of the heart and lungs to exercise on a stationary bicycle. There is no pass or fail. Exercise capacity has a big influence on the need for support of the major body systems during and after an operation. The results of the exercise test guide the anaesthetist, surgeon and other doctors caring for the patient.
CT Scan
This X-ray is used to look at your liver, other organs and the blood vessels going to and from your liver. It is used to determine the size of the liver, presence of liver cancers and any other abnormalities. Some abnormalities of blood vessels may make transplant surgery more complicated or in some cases impossible to proceed with liver transplantation. Contrast dye is injected into your vein.
Echocardiogram
This is an ultrasound of your heart and assesses how well the different parts of your heart are working.
Electrocardiogram (ECG)
The electrical activity of the heart is recorded by placing electrodes over the chest, arms and legs. An ECG will identify any disturbances in the heart’s rhythm and helps detect underlying heart disease
Endoscopy
A flexible tube with a small camera is passed down your oesophagus, or food pipe into your stomach to determine if you have any enlarged veins called varices. Varices are a complication of liver disease. A sedative is given before the procedure. You need to fast for 6 hours before the procedure. The procedure takes about 15 minutes.
Endoscopy and Variceal Banding, or Gluing
Varices are large veins usually found in the oesophagus and/or stomach. Varices may rupture and cause major bleeding so that you need urgent treatment which is given at the time of endoscopy.
Banding of oesophageal varices involves placement of rubber bands over the varices at the time of endoscopy. Gluing is usually kept for stomach varices. Glue is injected into the stomach varices causing the blood in the varices to clot and eventually the treated varix will disappear. Sometimes it is not possible to know which treatment will be necessary until the time of endoscopy.
The variceal banding procedure is usually repeated every 2 to 3 weeks until the varices are treated or eradicated. It usually takes 3 to 4 treatment sessions.
Hepatology
The study of liver disease.
Hepatologist
A doctor who specialises in the care of the liver.
MRI (Magnetic Resonance Imagery)
Images of your body are produced through a combination of computers, a powerful magnet and radio waves. The images are similar to those of a CT scan. You will be asked to remove all metal objects before entering the
scanner, which is shaped like a cylinder. If you have any metal in your body from previous operations make sure you tell the doctor. It is important to remain very still throughout the whole procedure.
Pulmonary function test: Spirometry, respiratory function tests
These tests examine your breathing and lung capacity and give us a baseline recording of your lung function.
Swabs MRSA/VRE
Swabs are collected from inside your nose, groin and around your anus to test for micro- organisms resistant to antibiotics.
Ultrasound
A picture is created by reflected sound waves from an instrument that is moved across the skin. The doctors will be particularly interested in your liver, bile ducts and the blood vessels that supply blood to and from the liver.
24-hour urine collection
Urine is collected for 24-hours to test renal function. The urine will need to be collected in a bottle or pan and transferred into a special bottle.
Liver Transplant Evaluation and Assessment Guide,
25 Nov 2022,
[https://oss-uat.clients.squiz.net/health/services/specialists/queensland-liver-transplant-service/liver-transplant-evaluation-and-assessment-guide]
This document is uncontrolled when printed. Before using the information in this document you should verify the current content on https://oss-uat.clients.squiz.net/health/services/specialists/queensland-liver-transplant-service/liver-transplant-evaluation-and-assessment-guide.