Antenatal information Guide
Your antenatal visits are a great way to learn how your baby is growing and what is happening to your body.
Due to COVID-19, prenatal visits might be different. Some doctors and midwives are using telehealth to see pregnant women. More information: COVID-19: information for pregnant and breastfeeding women.
During visits:
- your blood pressure will be checked
- the doctor or midwife will palpate (feel) your abdomen to see how much your baby has grown and listen to your baby’s heartbeat
- sometimes you may be weighed, have blood taken for tests and may have your urine checked.
-
Your care during pregnancy
-
Antenatal visits
Your antenatal visits are a great way to learn how your baby is growing and what is happening to your body.
Due to COVID-19, prenatal visits might be different. Some doctors and midwives are using telehealth to see pregnant women. More information: COVID-19: information for pregnant and breastfeeding women.
During visits:
- your blood pressure will be checked
- the doctor or midwife will palpate (feel) your abdomen to see how much your baby has grown and listen to your baby’s heartbeat
- sometimes you may be weighed, have blood taken for tests and may have your urine checked.
Your due date
A normal pregnancy lasts 37–42 weeks.
The average length of pregnancy is 280 days or 40 weeks, from the first day of your last menstrual period.
The medical term for the due date is ‘estimated date of delivery (EDD)’.
Did you know that only about 4% of women give birth on their baby’s due date!
More information: Better Health Channel – Baby due date
When do I see my doctor or midwife?
At your first appointment with your doctor or midwife, you will plan on who to see and when. Your appointments will generally follow the recommended antenatal schedule, shown in your Pregnancy Health Record.
Due to COVID-19, prenatal visits might be different. Some doctors and midwives are using telehealth to see pregnant women.
Things to ask at your visits
Ask your doctor or midwife about:
- results of tests and investigations
- smoking, alcohol and drug use
- managing back or pelvic pain
- premature labour - what to look out for
- who and when to call when you’re in labour
- labour and birth - what to expect and making a birth plan
- planning for your hospital stay and going home with your baby.
For after your baby is born, ask your doctor or midwife about:
- tests for your baby – including the Healthy Hearing and Neonatal Screening Tests
- Vitamin K injection for newborns
- immunisations for yourself and your baby
- breastfeeding
- the importance of ‘rooming in’
- skin to skin contact
- where to get help with breastfeeding.
Who can I call to ask questions?
Your doctor, midwife, or obstetrician is usually the best place to start.
Other contacts:
- 13 HEALTH: 13 43 25 84
- Child Health Services, Queensland Health
- Pregnancy, Birth and Baby Helpline: 1800 882 436
- True Relationships and Reproductive Health
- Australian Breastfeeding Association: 1800 686 268
- Lifeline: 13 11 14
More contacts are listed in your Pregnancy Health Record.
-
Routine tests during pregnancy
Your doctor or midwife will discuss the routine blood tests offered in pregnancy.
These tests are performed to check for anything that may cause problems during pregnancy or after the birth.
Other tests may include a:
- pap smear
- breast check.
More information: Pregnancy Birth and Baby – Blood tests during pregnancy
What if I have a negative blood group?
There are four main blood groups. A, B, AB, and O.
A blood test in early pregnancy tells you which blood group you are, and whether you are Rh positive or Rh negative. Most women (85%) are Rh positive.
If you are Rh negative and your baby is Rh positive it can cause health problems which can be treated.
You will be offered an Anti-D injection at 28 weeks and at 34 weeks of your pregnancy.
You will also be offered an Anti-D injection if you have:
- any vaginal bleeding during your pregnancy
- a miscarriage
- an abortion
- if you have been involved in an accident involving major force to the abdomen
- a medical procedure such as chorionic villous sampling (CVS) or amniocentesis.
You will also require a blood test following birth and may be given an Anti-D injection within 72 hours of your baby's birth if your baby is Rh positive.
More information: Queensland Clinical Guidelines, Parent Information - RhD negative blood type in pregnancy
Testing for gestational diabetes
Gestational diabetes only develops in pregnancy.
The condition occurs in two to three of every 100 pregnant women.
How do I find out if I have gestational diabetes?
Due to COVID-19, testing for gestational diabetes might be different to what is usually done.
If you have risk factors for gestational diabetes you will be offered a blood test in the first trimester.
All other women will be offered a blood test around 24–28 weeks of pregnancy. You may have to have a second test where you are given a special glucose drink and have blood samples taken over two hours.
Your doctor or midwife will discuss what is best for you.
For more information about gestational diabetes visit:
-
Ultrasounds during pregnancy
Antenatal ultrasound scans are recommended at certain points during pregnancy to check the:
- number of babies you’re expecting—single, twins or more
- age of your pregnancy (in a dating scan)
- your baby's growth and physical development
- position of the placenta
- length of the cervix (neck of the womb).
We also use scans to monitor:
- the amount of amniotic fluid around the baby
- the health and function of the placenta, which supports your baby’s growth
- any complications, such as bleeding, fluid loss, high blood pressure (hypertension) and diabetes in pregnancy.
Learn more about routine tests and your care during pregnancy.
When you need an ultrasound
Your doctor or midwife will advise you when an ultrasound may be recommended. The following ultrasounds are common in pregnancy.
8–9 weeks dating scan
An early ultrasound at around 8 to 9 weeks is considered to be the best time to confirm the due date, ensure the pregnancy is in the uterus (womb) or for reassurance.
11–13 weeks first trimester screen
An ultrasound (also known as a nuchal translucency scan or early structural assessment) is recommended for all pregnant women. If combined with a blood test (free Beta-HCG and PAPP-A), it can be used to generate a risk for chromosomal abnormalities called a combined first trimester screen.
This is a screening test that will calculate your estimated risk of having a baby with Down syndrome and other chromosomal abnormalities. This ultrasound scan also helps to exclude any major structural abnormalities of your baby early in pregnancy and can be used to screen for preterm preeclampsia if this is offered.
If you decide to use a blood test for genetic screening such as NIPT, it’s also very important to check for physical abnormalities of your baby by having this ultrasound.
18–20 weeks morphology scan
This is an important ultrasound used to rule out major physical abnormalities in your baby and check the location of the placenta.
It is also important to check the length of your cervix at this scan as a short cervix predicts preterm birth. Most parents know this scan as 'the one where we may find out the baby’s sex'.
Where to go for your ultrasounds
You’ll need a referral from a health professional.
You can have your ultrasounds done at a radiology clinic. In some cases, you may be referred to a hospital. Use service finder on the Health Direct website to find your nearest a radiology service.
There may be a charge for your ultrasound depending on where you have it. Some will bulk bill through Medicare. Please talk to a health professional if you can’t pay out of pocket expenses for an ultrasound.
-
Common discomforts in pregnancy
Your body is undergoing many changes during pregnancy and you may experience some health issues along the way.
Many of these issues are a normal part of pregnancy. If you are concerned, talk to your doctor or midwife.
Common discomforts during pregnancy may include:
- morning sickness and severe vomiting
- cramps in your legs and feet
- urinary frequency (needing to pass urine often)
- urinary stress incontinence (leaking urine)
- heartburn and indigestion
- blocked nose
- varicose veins (swollen veins) in your legs
- varicose veins in the genital area
- constipation and haemorrhoids
- backache
- vaginal thrush
- infections (influenza, chickenpox, shingles, slapped face, whooping cough).
More information:
- Pregnancy health problems: what’s common, what’s not
- Common health problems in pregnancy
Sickness and vomiting in pregnancy
You can read these helpful tips for managing morning sickness and find out more information on severe vomiting during pregnancy.
Next section: Looking after yourself and your baby
-
Looking after yourself and your baby
-
Healthy eating during pregnancy
During pregnancy it is important for both you and your baby that you eat well. Your choices of what to eat and drink at this time can affect your health and the health of your baby for many years to come.
There is only a small increase in the amount of food you need to eat while you are pregnant.
However, you do need more of certain nutrients, so it is very important that you make good choices for a nutritious diet.
Important nutrients
Folate (or folic acid) during pregnancy.
Folate is needed for the growth and development of your baby. It is especially important in the month before you fall pregnant and the first trimester (three months) of pregnancy.
A good intake of folate reduces the risks of your baby being born with some abnormalities such as spina bifida (a disorder where the baby’s spinal cord does not form properly).
Dietary sources high in folate include:
- green leafy vegetables – such as broccoli, spinach, bok choy and salad greens
- some fruits – such as avocado, orange, papaya and banana
- cereals and breads with added folic acid.
How much folic acid do you need?
Women planning a pregnancy and in the early stages of pregnancy should eat a variety of folate-containing foods. You should also take a folic acid supplement of 400 micrograms per day at least one month before, and three months after, you become pregnant.
Iron
You need more iron during pregnancy. If you do not have enough iron, you may develop anaemia.
Good sources of iron include:
- lean red meat, pork, chicken and fish
- wholegrain breads and cereals, legumes and green leafy vegetables.
If you are low in iron, your doctor or midwife may suggest taking an iron supplement (tablet or liquid).
You can help your body get iron from the food you eat or drink by:
- including vitamin C with meals (e.g. citrus fruits, tomato, capsicum)
- including animal protein with green leafy vegetables at a meal
- using antacids sparingly.
How much iron do you need?
Pregnant women need 27 mg iron each day. Pregnant women should not eat more than 45 mg iron each day.
Iodine
Adequate iodine in pregnancy is essential for your baby’s growth and brain development.
Iodine is important for your baby’s development in the womb.
Good food sources of iodine include:
- vegetables
- bread with added iodine
- seafood
- eggs.
How much iodine do you need?
Pregnant women should take a supplement containing 150 micrograms of iodine each day.
Multivitamins
A multivitamin during pregnancy is not necessary unless you do not have a balanced diet. Compare what you are eating with the following food group table.
Remember, a folic acid supplement is important during the first trimester of pregnancy, and iodine is essential during pregnancy (and breastfeeding). You may also need to take an iron supplement if your iron levels are low.
You may choose to get these nutrients from individual tablets or from a multivitamin.
Always check with your doctor or midwife before taking any supplements, as an excessive intake of these can be harmful and reduce the absorption of other nutrients.
More information: Queensland Health Nutritional Education Materials Online (NEMO)
Food groups
Food group
Serves per day
(for 19-50 year olds)
1 serve equals
Vegetables and legumes/beans
5
½ cup cooked green or orange vegetables (e.g. broccoli, carrot, pumpkin or spinach)
½ cup cooked, dried or canned beans, chickpeas or lentils (no added salt)
1 cup raw leafy green vegetables
½ medium potato, or other starchy vegetable (sweet potato, taro, or cassava)
½ cup sweet corn
75g other vegetables (e.g. 1 small-medium tomato)
Fruit
2
1 piece medium sized fruit (e.g. apple, banana, orange, pear)
2 pieces smaller fruit (e.g. apricot, kiwi fruit, plums)
1 cup diced, cooked or canned fruit
½ cup 100% juice
30g dried fruit (e.g. 1½ tbsp sultanas, 4 dried apricot halves)
Grain (cereal) foods - mostly wholegrain
8½
1 slice of bread
½ medium bread roll or flat bread
½ cup cooked rice, pasta, noodles, polenta, quinoa, barley, porridge, buckwheat, semolina, cornmeal
⅔ cup breakfast cereal flakes
¼ cup muesli
3 crisp breads
1 crumpet or 1 small English muffin or scone
Lean meat and poultry, fish, eggs, nuts and seeds, and legumes/beans
3½
65g cooked lean red meats (e.g. beef, lamb, pork, venison or kangaroo) or ½ cup lean mince, 2 small chops, 2 slices roast meat
80g cooked poultry (e.g. chicken, turkey)
100g cooked fish fillet or 1 small can fish, no added salt, not in brine
2 large eggs (120g)
1 cup (170g) cooked dried beans, lentils, chickpeas, split peas, canned beans
170g tofu
⅓ cup (30g) unsalted nuts, seeds or paste, no added salt
Milk, yogurt, cheese and/or alternatives - mostly reduced fat
2½
1 cup (250ml) milk
40 g (2 slices) hard cheese (e.g. cheddar)
120g ricotta cheese
200g yoghurt
-
How much weight should I gain?
The weight you should aim to gain will depend on what your body mass index (BMI) was before you became pregnant. Use this tool to calculate your BMI.
Your BMI is the number used to work out your recommended amount of weight gain.
Pre-pregnancy BMI
Recommended total gain
Weekly guide in 2nd and 3rd trimester
Less than 18.5 kg/m²
12½ to 18kg
1/2 kg per week
18.5 to 24.9 kg/m²
11½ to 16kg
400g per week
25 to 29.9 kg/m²
7 to 11½ kg
Less than 300g per week
Above 30 kg/m²
5 to 9kg
Less than 300g per week
Pregnancy Weight Gain charts
You may find it easier to follow a pregnancy weight gain chart. The charts are divided in two groups:
- Pregnancy weight gain chart for BMI less than 25kg/m2
- Pregnancy weight gain chart for BMI 25kg/m2 or over.
More information: How much weight should I gain while pregnant.
-
Food Safety in pregnancy
Listeria in pregnancy
Listeria is a bacteria found in some foods, which can cause an infection called listeriosis. If passed on to your unborn baby it can cause premature birth, miscarriage or damage. Throughout your pregnancy, it is important to avoid foods that have a high risk of containing listeria.
Foods that might contain Listeria and should be avoided include:
- unpasteurised dairy products
- soft cheeses such as brie, camembert, ricotta, and fresh fetta, unless they are cooked (yellow, hard cheese, and processed packaged cheese are safe)
- soft serve ice cream and thick shakes
- all paté
- ready-to-eat cold meats, including deli and packaged meats (e.g. ham, salami, cooked chicken)
- ready-to-eat salads (from salad bars, buffets, supermarkets etc.)
- raw or smoked seafood (including oysters, salmon, sashimi, sushi)
- undercooked meats (e.g. raw steak) and eggs
- ready to eat prawns.
Eating fish during pregnancy
Fish is a safe and important part of a healthy diet. It is an excellent source of protein, low in saturated fat, high in omega 3 fish oils and a good source of iodine.
However, some types of fish should be restricted as they may contain higher levels of mercury.
Recommendations for pregnant women
(1 serve = 150g)
1 serve per fortnight of shark (flake) or billfish (swordfish/broadbill and marlin) and NO other fish that fortnight
or
1 serve per week of Orange Roughy (Deep Sea Perch) or catfish and NO other fish that week
or
2–3 serves per week of any other fish and seafood not listed above.
Eating eggs during pregnancy
Do not eat raw or undercooked eggs. Eggs must be cooked through so that both the white and yolk are hard.
Food safety tips
Here are some tips for keeping your food safe:
- choose freshly cooked and freshly prepared food
- thaw food in the fridge or defrost in the microwave
- cool left-over food in the fridge, rather than the bench
- wash your hands, chopping boards and knives after handling raw food
- make sure hot food is very hot (above 60 degrees Celsius) and cold foods are very cold (below 5 degrees Celsius) – both at home and when eating out
- make sure all food is fresh and eaten within the use-by date
- wash fruits and vegetables thoroughly before use
- eat leftovers within 24 hours and reheat foods to steaming hot
- heat leftovers to above 74 degrees Celsius, for at least two minutes
- cook all meat, chicken, fish, and eggs thoroughly
- never re-freeze food once it has been thawed or reheated.
More information on healthy eating during pregnancy, including fact sheets and resources suitable for Aboriginal, Torres Strait Islander, Maori, and Pacific Islander women are available through Queensland Health Nutritional Education Materials Online (NEMO).
-
Exercise during pregnancy
It’s great to be active and stay fit while you’re pregnant.
Check with your doctor or midwife to make sure there are no health problems to prevent you from exercising.
If there are no problems, try to do 30 minutes of moderate exercise (like walking) on most days of the week.
Regular exercise can help you:
- stay at a healthy weight
- relax
- be stronger and fitter – which is good for coping with pregnancy, labour and being a parent
- decrease discomforts like back pain and varicose veins – which can affect some pregnant women.
If you haven’t been physically active before
Pregnancy can increase your risk of injury because your joints loosen up to let your body grow and make it easier to give birth.
You can prevent injury in pregnancy by avoiding high impact exercise like jumping up and down, repetitive bouncing movements, and any movements that over-stretch your hip, knee, ankle or elbow joints.
Stop exercising if you experience:
- dizziness
- vaginal bleeding
- contractions
- pain
- shortness of breath
- decreased baby movements
- “waters are leaking”.
Read more information on pregnancy and exercise.
Pelvic floor exercises
By performing pelvic floor exercises, you can strengthen muscles to help reduce or avoid stress incontinence after pregnancy.
Incontinence is a common but treatable condition – view the video below or visit the Continence Foundation of Australia for more information.
To learn safe exercises, you can download a copy of Pelvic floor health for expectant and new mums from the Continence Foundation of Australia.
One in three women who ever had a baby wet themselves - consumer education video
This video answers the question about why a woman has an increased risk of leaking urine (urinary incontinence) after childbirth. Find out how to prevent this from happening, how to treat the condition and where to get help.
-
Perineal massage
From about 35 weeks you can start preparing for your labour and birth with perineal massage.
Research has shown that massaging the perineum during late pregnancy may encourage elasticity and reduce the risk of tearing during childbirth.
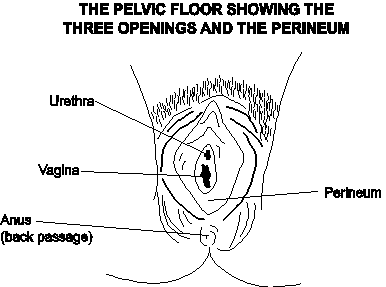
Where is my perineum?
The perineum is the area between the vaginal opening and anus. Some women choose to use perineal massage as a way of (hopefully) reducing their risk of perineal trauma during childbirth.
When can I start perineal massage?
You can start massage from about 35 weeks and perform no more than three times per fortnight.
How should I do perineal massage?
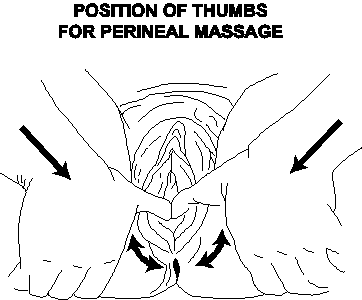
- Gently insert thumbs or 1-2 fingers, 3-5 cm into the vagina, and firmly sweep in a downward and side to side motion for five minutes, using a natural oil for lubrication, (Avoid nut-based oils if known allergies. Do not use baby oil, mineral oil or petroleum jelly).
- You may feel a burning sensation which will diminish over time.
- Do not massage if you have active genital herpes or a vaginal infection present.
- Most women consider their partner’s involvement as positive.
Ask your doctor or midwife for more information.
-
Medications, alcohol, and smoking during pregnancy
Medications
Not all medicines are safe during pregnancy and breastfeeding.
This includes medicines that are prescribed, natural supplements, or over the counter from the pharmacy or supermarket.
Make sure you tell your doctor or midwife, and pharmacist, about all the medicines you are taking – especially if you:
- have an existing medical condition
- are taking an over the counter or prescribed medication
- are taking alternative and complementary therapies
- are using illicit drugs - seek urgent advice from a health professional.
More information: Queensland Clinical Guidelines – Using drugs in pregnancy
Drinking alcohol during pregnancy
The safest choice for your baby is to not drink any alcohol.
The risk of damage to your baby increases the more you drink, and binge drinking is especially harmful.
There is no safe amount of alcohol to drink when you’re pregnant.
What if you drank before you knew you were pregnant?
If you drank small amounts of alcohol before you knew you were pregnant, be reassured that the risk of harm to your baby is low.
More information: The National Organisation for Fetal Alcohol Syndrome. Alcohol and Pregnancy
Smoking during pregnancy
Stop smoking during pregnancy and you and your baby will immediately feel the benefits.
Toxic chemicals are absorbed into your bloodstream and passed on to your baby through the umbilical cord. If you are unable to stop smoking, cut down as much as you can.
Smoking while pregnant increases your risk of:
- ectopic pregnancy
- miscarriage
- premature labour
- complications during birth.
- sudden infant death syndrome (SIDS)
- low birth weight
- infections and other health problems
- asthma and other breathing difficulties
- behavioural problems.
Smoking while pregnant can increase your baby’s risk of problems after they are born:
For advice and support visit Quit HQ or call Quitline on 13 78 48.
More information: Pregnancy Birth and Baby - Smoking and pregnancy
Helpful hints to stop smoking
When you feel the urge to smoke:
- distract yourself for five to 10 minutes so the craving can pass
- relax and take some deep breaths
- drink a glass of water
- call a friend
- practice your pelvic floor exercises
- change the habits you associate with smoking
- take it a day at a time and reward yourself for success
- visit Quit HQ or call Quitline on 13 78 48.

More information: Coping with quitting and staying smoke- and vape-free
-
Vaccinations during pregnancy
Immunisation is a simple and effective way to protect yourself and your baby from certain infections.
During pregnancy, it is recommended that you have the following vaccinations.
‘Flu’ (Influenza)
Influenza can cause serious illness and being pregnant increases the risk of influenza complications, especially with the H1N1 influenza virus. Influenza vaccine is safe and can be administered before, during or after pregnancy.
Whooping cough (Pertussis)
Whooping cough can cause serious illness and even death in babies less than six months old. It is now recommended that all pregnant women receive a pertussis (whooping cough) vaccination during their third trimester (ideally at 28 weeks) of every pregnancy.
Other vaccinations
Check with your doctor whether you have immunity against measles, mumps, rubella, chickenpox – as well as influenza and whooping cough.
More information:
-
Infections and precautions in pregnancy
Coronavirus and pregnancy
Coronavirus (COVID-19) is a new virus and we are still learning how it may affect you and your baby.
To reduce your chance of getting the virus, follow these prevention measures:
- wash your hands regularly and frequently—use soap and water for 20 seconds or alcohol-based hand sanitiser/gel
- use social and physical distancing (stay 1.5 metres away from other people)
- avoid anyone who has a fever, cough or symptoms of a cold or chest infection
- avoid touching your eyes, nose and mouth.
Cytomegalovirus
Read about the common viral infection cytomegalovirus (CMV).
Gardening during pregnancy
It is important to wear gloves when gardening and wash hands afterwards.
Toxoplasmosis
Cats can be a source of Toxoplasmosis—a serious infection that can cause defects or death in your baby. It is important to avoid contact with cats and use gloves when handling cat litter.
Next section: Mental wellbeing during pregnancy
-
Mental wellbeing during pregnancy
Pregnancy, birth and early parenthood are times of great change.
During pregnancy most women experience a range of emotions. Your pregnancy hormones may make you more emotional than usual. You may worry about whether your baby will be normal and how you will cope with labour. It helps if you can talk openly about any concerns with your partner or a close friend.
Common concerns of pregnant women can be:
- will my baby be normal?
- worrying about labour
- changing body, emotions and relationships.
Read more about pregnancy and new parents and visit Dear Mind for many ways to strengthen your mental wellbeing.
Depression and anxiety during pregnancy
Depression and anxiety can occur at any time in your life and can often come to the surface with major events like pregnancy or having a baby.
Around 12% of pregnant women in Australia experience antenatal depression (depression during pregnancy). The risk is higher if you have been depressed in the past.
It is important to keep a check on how you are feeling emotionally and discuss any concerns with your health professional. Let someone know if you are:
- feeling low, anxious or tense very often
- feeling guilty
- feeling that things are hopeless
- not enjoying things you normally do
- crying all the time
- irritable
- finding it hard to sleep, concentrate or make decisions
- wanting to harm yourself.
Read more on perinatal anxiety or find a health professional at Beyond Blue.
Mental wellbeing for partners
Partners share many of the experiences of pregnancy.
Partners also experience the worries, problems, pleasure, and the waiting. Sometimes partners may also have issues of their own to work out.
You can read and share information from Dad’s guide to fatherhood and Dads guide to pregnancy.
There is also information in many languages from the Multicultural Health Communication Service.
Where to get help
If you or someone you know is showing signs of depression or anxiety, there are places you can go to for help.
Pregnancy, Birth and Baby Helpline: 1800 882 436
Beyond Blue – Pregnancy and new parents: 1300 224 636
MUMspace – support for the emotional health of new mums, at every step.
Prenatal Anxiety and Depression Australia (PANDA): 1300 726 306
Lifeline: 13 11 14
Mensline Australia: 1300 789 978
Sane Australia Helpline: 1800 18 7263
White Cloud Foundation: 1300 702 926
-
Depression and anxiety during pregnancy
Depression and anxiety can occur at any time in your life and can often come to the surface with major events like pregnancy or having a baby.
Around 12% of pregnant women in Australia experience antenatal depression (depression during pregnancy). The risk is higher if you have been depressed in the past.
It is important to keep a check on how you are feeling emotionally and discuss any concerns with your health professional. Let someone know if you are:
- feeling low, anxious or tense very often
- feeling guilty
- feeling that things are hopeless
- not enjoying things you normally do
- crying all the time
- irritable
- finding it hard to sleep, concentrate or make decisions
- wanting to harm yourself.
Read more on perinatal anxiety or find a health professional at Beyond Blue
-
Mental wellbeing for partners
Partners share many of the experiences of pregnancy.
Partners also experience the worries, problems, pleasure, and the waiting. Sometimes partners may also have issues of their own to work out.
You can read and share information from Dad’s guide to fatherhood and Dads guide to pregnancy.
There is also information in many languages from the Multicultural Health Communication Service.
-
Where to get help
If you or someone you know is showing signs of depression or anxiety, there are places you can go to for help.
- Pregnancy, Birth and Baby Helpline: 1800 882 436
- Beyond Blue: 1300 224 636
- Perinatal Anxiety and Depression Association (PANDA): 1300 726 306
- Lifeline: 13 11 14
- MensLine Australia: 1300 78 99 78
- Sane Australia - Support services: 1800 18 7263
- White Cloud Foundation: 1300 702 926
- Black Dog Institute
- MUMspace
Next section: Journey of labour
-
Journey of labour
-
Preparing for labour and birth
In addition to the natural physical preparation your body makes for birth, you may also find yourself preparing emotionally.
You may:
- feel a strong need to be ready
- find yourself worrying more than usual
- be concerned about making it through labour, or whether your waters will break in public
- be concerned about whether your partner will be able to help you, or whether you will have a bowel movement during the birth and how your partner might react to that
- be worried about the safety of you and your baby during birth
- be worried about having a caesarean birth.
These concerns are common. Discuss your concerns with your midwife or doctor, so you can feel prepared and informed before labour starts.
Your birth preferences
Preparation for labour starts during pregnancy.
Your birth preferences (sometimes known as a birth plan) is a written list of what you would like to happen when you are in labour and give birth.
Birth preferences may include:
- who you would like with you in labour
- what position you would like to give birth in
- what comfort measures you might use as your pain relief options.
It is important to stay flexible
Remember that things may not go according to plan.
There may be complications, or you may change your mind about something. Think about what is important to you for your birth.
Other questions to consider when deciding on your birth preferences may be:
- what if I need a caesarean birth?
- what is the usual practice for an induction of labour?
- what equipment may be used in my labour and for the birth of my baby, and why?
- do I have any cultural or religious needs around giving birth?
- can I expect to hold my baby skin-to-skin after he/she is born?
More information: Pregnancy, Birth and Baby - Making a birth plan
-
Who will support you in labour
It can be helpful to have people around you who can provide both emotional and physical support during labour.
Hospitals usually allow two support people with you in labour. This could be your partner, another family member or a friend.
- Some women choose to hire a doula or birth attendant to support them during labour.
- A doula is not a member of your maternity team but is experienced in supporting women and their partners during labour.
- You can check with your midwife or doctor regarding policies about support persons.
Studies show that women who have someone with them right through labour have a more positive experience of labour and are less likely to need medication for pain relief.
Please note: Due to COVID-19, the number of support people you can have with you during labour and birth may be limited. It is suggested that you choose someone who can stay with you for the whole time.
Being a birth partner
There are many things a birth partner can do to provide support.
They can:
- keep you company and help to pass the time during the early stages
- hold your hand, wipe your face, give you sips of water
- massage your back and shoulders, help you to move or change position, or anything else that helps
- comfort you as your labour progresses and your contractions get stronger
- remind you how to use relaxation and breathing techniques, perhaps breathing with you if it helps
- support your decisions, such as the pain relief methods that you choose
- help you explain to the midwife or doctor what you need – and the other way around – which can help
- help you feel much more in control of the situation
- (if possible) cut the umbilical cord – you can talk to your midwife about this.
More information: Pregnancy, Birth and Baby – Being a birth support partner
-
How your body prepares for labour
Your body is getting ready for childbirth throughout your pregnancy, especially in the last few weeks with final preparation.
The pelvis is made up of two large bones joined by cartilage and ligaments – at two joints in the woman's lower back at the sacrum (called the sacroiliac joints) and at the front symphysis pubis bone.
During late pregnancy a hormone softens and relaxes these ligaments. This gives the pelvic bones the ability to stretch and open more easily for the birth of your baby. It is common in late pregnancy to experience lower back pain, or you may notice that you have a ‘pregnancy waddle’ when walking, due to these changes.
Braxton Hicks contractions
Braxton Hicks are also called ‘practice contractions’ because they are preparation for labour.
Braxton Hicks contractions can begin as early as the second trimester. However, they are most commonly experienced in the third trimester. When this happens, the muscles of the uterus tighten for approximately 30 to 60 seconds and sometimes as long as two minutes. If you have concerns or think you might be in labour, contact your midwife or the hospital.
Braxton Hicks are described as:
- irregular in intensity
- infrequent
- unpredictable
- non-rhythmic
- more uncomfortable than painful (although for some women Braxton Hicks can feel painful)
- they do not increase in intensity, or frequency
- they taper off and then disappear altogether
if your contractions are easing up in any way, they are most likely Braxton Hicks.
How your baby prepares for labour
Your baby may begin moving lower in the pelvis, which is called engagement.
How will I know if baby’s head is engaged?
You might notice this as increasing pressure in your lower abdomen, or you might notice that breathing becomes easier.
- For first time mothers, engagement usually occurs about 36 weeks of pregnancy.
- For second-time mothers, engagement may not occur until after labour begins.
Your baby is designed for the birth process
The baby's skull bones are divided into five plates that cross over during labour, making their head smaller by moulding to fit the birth canal. Mother and baby work together during labour.
-
Getting baby in the right position for birth
There are things you can do during pregnancy to encourage baby into the best position for labour.
How you sit and use your body can affect the position of your baby in the uterus.
While this does not matter so much during early pregnancy, later on it can affect the position that the baby moves into (in the pelvis).
Presentation during labour refers to which part of the baby enters the birth canal first. Normally, the crown of the head will enter first, which is known as cephalic presentation. Other forms of presentation such as breech presentation may cause difficulties with birth.
Once the baby is head down, the best position for a labour is the anterior position.
Anterior position means the baby’s head enters the pelvis facing your back.
This is the ideal and most common position for birth (see image). When baby is in the anterior position, the smallest dimension of the baby’s head leads the way through the birth canal.

What can I do to get my baby in the best position?
You can use different positions during your pregnancy to give you the best chance of ‘optimally positioning your baby’ prior to labour.
Positions include:
- hands and knees, for as long as comfortable, or sitting on the floor

- lying on your side is a better option when on the lounge, than sitting slumped and relaxed back into the lounge chair

- sitting on a low stool or fit ball, where you are in a supported squat.

What if baby is in the posterior position
Posterior position means the baby’s head enters the pelvis facing your stomach instead of your back.
It’s good to know that most babies will turn around during labour, but some don't.

How can this affect my labour?
If your baby is in the posterior position when labour starts, it can lead to a longer labour with more backache.
If baby doesn’t turn, you may be able to push baby out yourself or your doctor may need to turn the baby’s head and/or help your birth with forceps or a vacuum cup.
-
When to seek advice during pregnancy
Seek advice from your doctor or midwife, or come to hospital if you:
- have bright red, fresh blood loss
- feel your baby’s movements have changed, or you are worried about your baby’s movements
- feel unwell (flu like symptoms) or are experiencing a burning or stinging sensation when passing urine
- have severe back pain
- have uncontrollable diarrhoea and or vomiting
- feel your stomach is tender, or you experience severe indigestion pain that you have not had before
- feel faint or have fainted
- are experiencing signs of labour (call early if you have a planned caesarean birth).
IMPORTANT: Call the hospital any time, day or night, to speak with a midwife. You will be asked questions about what is happening. You can then plan when to come into hospital.
Bring your Pregnancy Health Record with you.
More information: Pregnancy, Birth and Baby – What happens to your body during childbirth
-
Final preparations for labour
For mother:
- have your bag packed for hospital from 36 weeks
- go through your birth preferences with your birthing partner(s) and doctor or midwife
- practice your pelvic floor exercises and do some gentle exercise.
For birth partner:
- keep a list of necessary telephone numbers
- check the route to the hospital and have money ready for car parking
- have a labour bag packed for yourself
- make sure your mobile phone is always fully charged.
What to bring to hospital
For mother:
- Pregnancy health record
- maternity bras
- two packs of maternity pads
- current medication
- own pillow (if desired) – labelled
- clothes for labour – old t-shirt, comfortable clothing, warm socks, old underwear, track pants for after birth
- massage oil or lotion
- spray bottle (non-aerosol) for cooling
- tissues and toiletries – soap, shampoo, toothpaste, tooth brush
- food such as barley sugar, jelly beans, fruit bars, glucose drinks
- thongs or slippers
- lip cream for dry lips.
For baby:
- two-dozen newborn size nappies
- six newborn singlets
- six newborn jumpsuits
- six to eight bunny rugs or cotton wraps
- baby wipes / cotton wool
- three face washers for baby bath.
Other:
- camera (charged)
- mobile phone or phone card
- music for use during labour
- baby car seat for discharge
- pen.
Next section: Stages of labour
-
Stages of labour
-
Baby’s journey of labour
The human pelvis has a complex shape, making your baby negotiate several manoeuvres during labour and birth.
Every mother’s pelvis is widest side to side at the entrance – because of this, most babies enter the pelvis looking left or right. The exit from the pelvis is widest from front to back, so babies almost always turn face up or face down.
These manoeuvres occur from forces of labour and the resistance provided by the birth canal. In addition to making these turning manoeuvres, the baby is simultaneously descending further down the vagina.
Finally, the top of your baby’s head appears (crowns), stretching your vaginal opening. When the vulva has stretched enough, the baby’s head will emerge – usually by extending the head, lifting its chin off the chest and thus emerging from under your pubic bone.
The baby usually emerges face down but will turn to one side very quickly as the shoulders turn to take the same route. The rest of the body is born and then you can hold your new baby!
-
Hormones during labour
Oxytocin: Known as the hormone of love, oxytocin is secreted during sex, after ovulation and during labour, birth and breastfeeding. It creates nurturing and loving feelings.
Endorphins: Endorphins are produced in response to pain and stress. Endorphins have calming and pain-relieving effects. As labour progresses and pain intensifies, endorphin levels steadily increase in unmedicated labours.
Adrenaline: Adrenaline is also known as the ‘fight or flight’ hormone. Adrenaline is secreted in response to stress, fear and extreme pain. If a woman experiences these feelings during labour, too much adrenaline may be produced which can slow labour.
More information: Hormones in labour: oxytocin and the others – how they work
-
Stages of labour
Labour is divided into four stages.
- The first stage of labour is the slow opening of your cervix.
- The second stage is the birth of your baby.
- The third stage is separation and birth of the placenta.
- The fourth stage is the first two hours after birth.
The main signs of labour starting are:
- contractions
- a ‘show’ (a mucous blood-tinged vaginal discharge)
- waters breaking.
-
First stage of labour
The first stage of labour is made up of three different phases and involves the thinning of the cervix and its dilation to around 10 centimetres.
Latent phase
- Generally, this stage is the longest and the least painful part of labour.
- The cervix thins out and dilates from zero up to four–six centimetres.
- This may occur over days or hours and be accompanied by mild contractions.
- The contractions may be regularly or irregularly spaced, or you might not notice them at all.
Active phase
- The next phase is marked by strong, painful contractions that tend to occur three or four minutes apart, and last from 30 to 60 seconds.
- The cervix dilates from four–six to eight centimetres.
Transition
- The cervix dilates from eight to 10 centimetres (that is, fully dilated).
- These contractions can become more intense, painful and frequent. It may feel as though the contractions are no longer separate but running into each other.
- It is not unusual to feel out of control and even a strong urge to go to the toilet as the baby’s head moves down the birth canal and pushes against the rectum.
Throughout the first stage of labour, careful monitoring and recording of your wellbeing, your baby’s wellbeing, and the progress of your labour, is important. This helps us to know whether your labour is progressing normally, to recognise any problems early and for clear communication. Ideally, you will experience the latent phase in the comfort of your home. You may wish to come to hospital as you move through the active phase.
More information: Queensland Clinical Guidelines parent information – Early labour
What can I do in the active stage of labour?
Birth partner’s role
- Remind your partner to go to the toilet.
- Help her with changing positions.
- It might help to dim the lights or play some music.
- Support her in any decisions she makes about pain relief.
- Keep yourself relaxed as possible and look after your needs.
- Sometimes humour can lighten the atmosphere when appropriate.
Helping yourself in first stage
- Stay well hydrated.
- Eat lightly during labour; your digestive system naturally moves more slowly, and you may find that you become nauseated. Some easily digested foods include fruits, yogurt or toast.
- Choose positions of comfort; you might find that your body instinctively moves to certain positions during contractions.
- Slow swaying movements may also help during contractions.
- Standing helps your body and your baby work with gravity and encourages the downward movement of your baby through the pelvis.
- Remember – an empty bladder is more comfortable and gives your baby more space to move down.
More information: Pregnancy, Birth and Baby – Giving birth - first stage of labour
-
Second stage of labour
The second stage of labour is the birth of your baby.
The second stage of labour starts when your cervix is fully dilated, and you will usually have a strong urge to push because of the pressure your baby’s head is placing on your pelvic area.
At this stage your baby is moving from your uterus into your vagina and out into the world.
The second stage can last from 10 minutes to two hours.
What can I do in the second stage?
Helping yourself during the second stage
- Push when you have a contraction and relax in between.
- It is more effective to get two or three pushes in with each contraction, breathing in between, rather than one long push.
- Being upright allows gravity to help you.
- Relax your pelvic floor muscles around the vaginal opening.
- Your midwife may apply warm compresses to your perineum for comfort and to reduce tearing.
Birth partner’s role
- Help your partner into a comfortable position.
- Your encouragement is important but avoid cheerleading.
- It can be helpful to repeat the midwife’s advice to your partner in a calm steady voice.
- Offer your partner sips of water or ice.
More information: Pregnancy, Birth and Baby – Giving birth - second stage of labour
-
Third stage of labour
After the birth of your baby, your uterus gently contracts to loosen and push out the placenta. This may occur five to 30 minutes after the birth of your baby.
The muscles of the uterus continue to contract to stop the bleeding. This process is always associated with a moderate blood loss – up to 500 millilitres. In this stage of labour, one of the potential problems is excessive bleeding (postpartum haemorrhage), which can result in anaemia and fatigue. This is why the third stage is carefully supervised.
There are two approaches to managing the third stage:
- natural (also known as physiological or expectant) management, or
- active management.
Natural third stage
What is a natural third stage?
A physiological or natural third stage means that you wait for the placenta to be delivered naturally.
After your baby's birth, your midwife will delay clamping the umbilical cord to allow oxygenated blood to pulse from the placenta to your baby.
Your uterus (womb) will contract, and the placenta will peel away from the wall of your uterus. The placenta will then drop down into your vagina, ready for you to push it out.
Delayed cord clamping
For baby
The benefits of delayed cord clamping for the baby include a normal, healthy blood volume for the transition to life outside the womb; and a full count of red blood cells, stem cells and immune cells which results in higher iron stores in the baby for up to six months.
For mother
Delayed clamping keeps the mother-baby unit intact and can prevent complications with delivering the placenta.
Active (or managed) third stage
Benefits of an active third stage
The advantage of an active third stage is the lower risk of very heavy bleeding immediately after the birth. Your midwife or doctor will recommend you have an active third stage if you had complications during pregnancy or labour, such as:
- twin pregnancy
- polyhydramnios
- heavy bleeding during pregnancy or in labour
- a history of retained placenta
- a low-lying placenta
- anaemia
- an induced or very long labour
- an assisted birth or caesarean birth.
Active third stage
Immediately after the birth of your baby, the midwife or doctor gives you (with your consent) an injection of oxytocin, clamps and cuts the umbilical cord, and then carefully pulls on the cord to speed up delivery of the placenta.
Modified active third stage
This is a combination of active and natural. It is similar to active third stage but it includes delayed cord clamping.
-
The fourth stage
Baby’s birthday
After the birth, you and your partner will be given time with your baby so that you can get to know one another.
- It’s important that you and your baby stay together, skin to skin, ideally for the first two hours after birth.
- Your baby will be examined, weighed, measured and given identification bracelet/s.
- If you consent, baby will also be given vitamin K as an injection or orally.
- Your baby may be dressed and wrapped in a warm blanket.
- You may then be transferred to the postnatal wards or you may request an early discharge if you and baby are well.
Checks after your baby is born
While you are holding your baby, your midwife or doctor will do a check called an ‘APGAR score’.
The APGAR score will be done twice, at one minute and five minutes after birth. You probably won’t even notice it’s being done, as the midwife can do this while baby and mother are skin to skin.
It helps the midwife or doctor to know whether your baby needs additional care following birth.
The APGAR score is based on the baby’s:
- breathing rate
- heart rate
- skin colour
- muscle tone
- reflexes.
Blood loss after birth
Blood loss after birth is normal.
Bleeding in the days or weeks after birth (also called lochia) is completely normal and occurs regardless of whether you have a vaginal birth or caesarean birth.
What is normal blood loss after birth?
Women’s experiences of bleeding after birth vary considerably. In the first few days after birth, most women experience moderate to heavy bleeding. Over the first few days to weeks this bleeding will gradually decrease and will change colour.
Most women will stop bleeding between four and six weeks after birth. It is also common for bleeding to be heavier after breastfeeding.
More information: Queensland Clinical Guidelines parent information – Bleeding after birth
Next section: Birth - frequently asked questions
-
Birth - frequently asked questions
-
When does labour start?
A normal pregnancy lasts 38–42 weeks.
Every labour and birth is different. It is still not known exactly what happens to start labour.
The average length of pregnancy is 280 days or 40 weeks, from the first day of your last menstrual period. The medical term for the due date is estimated date of delivery (EDD).
Did you know that only about four percent of women give birth on their baby’s due date!
-
When will my waters break?
Most women’s waters break during labour, but it can also happen before labour starts.
When your waters break, the amniotic sac breaks, and the fluid drains out through your vagina. It can be a gush or a slow trickle.
The fluid will usually be clear but can be yellow or straw coloured. If it is green or red in colour, there may be a problem.
What should I do when my waters break?
Whatever the colour, you should put a pad on and call your midwife or the hospital who will advise you on when to come into hospital.
-
How long does labour last?
All labours are different. Every labour is unique. The length of each person’s labour is different.
How quickly your labour progresses will depend on the baby descending (going down through the pelvis) and the cervix dilating (opening up) with strong, regular contractions.
On average for your first baby, the:
- first stage of labour can last from 10 to 14 hours
- second stage of labour can take one to two hours to push your baby out
- third stage can last five to 45 minutes
- fourth stage is the first two hours after birth.
If you have had a baby before, the:
- first stage of labour can last from five to eight hours
- second stage can last from five minutes to an hour.
-
What is pre-labour?
For up to a week before labour starts, you may notice that your body is preparing for labour.
Some women will notice:
- an increase in vaginal discharge (clear)
- a plug of mucous (‘show’) may be released from the cervix – perhaps with a streak of blood
- feeling unusually energetic (nesting instinct)
- frequent Braxton Hicks ‘practice’ contractions.
-
What do contractions feel like?
Women describe and experience contractions in different ways.
They may feel like:
- lower abdominal cramps that feel like period pain
- persistent dull lower backache
- inner thigh pain that may run down your legs.
At first these contractions are short and may be far apart – sometimes as much as 30 minutes apart.
As your labour progresses, they will get longer, stronger and closer together; until they last for about a minute and are coming faster, about every two or three minutes.
-
How do I time contractions?
From the beginning of one contraction until the next one begins. You can also time how long the contractions last.
The frequency of your contractions
Using a watch or clock, measure the frequency of your contractions by timing them from the beginning of one to the beginning of the next.
True labour will develop into a regular pattern, with your contractions growing closer together. In false labour, contractions remain irregular.
The length of your contractions
Measure the duration of each contraction by timing when it begins and when it stops. True contractions last about 30 seconds at the onset and get progressively longer up to 75 seconds and stronger. False labour contractions vary in length and intensity.
-
When do I come to hospital?
Seek advice or come to hospital if:
- Your waters break – put on a sanitary pad, note the time, the colour and amount of water then call your midwife or the hospital.
- Your contractions become painful, regular and are occurring at least five minutes apart (this timing will depend on your personal history, circumstances and will be discussed in your pregnancy).
- Labour has commenced and you have been advised to attend hospital early.
- You are experiencing signs of labour and you have a planned caesarean birth.
- You have a known medical or pregnancy condition that means you will require closer monitoring than usual in labour
- Your baby’s movements have changed, or you are worried about your baby’s movements.
Call ‘000’ for an ambulance if:
- You think your labour is progressing very quickly and you won’t make it to hospital.
- You experience heavy bleeding (similar to first day of a period) or have a severe headache and blurred vision.
-
What do I bring to hospital?
See ‘Final preparations for labour’.
-
What happens when I get to hospital?
When you arrive, a midwife will talk about what is happening to you and discuss your birth preferences.
The midwife will:
- ensure you have an identification band on your wrist
- check your temperature, pulse and blood pressure
- check the baby’s position by feeling your abdomen
- listen to the baby’s heart rate
- time your contractions
- with your consent, may do an internal (vaginal) examination to see how much your cervix has opened, and to check the baby’s position.
-
What if my labour is progressing slowly?
What can I do if labour is progressing slowly?
It’s good if you can relax and stay calm – anxiety can slow things down.
The midwife may suggest:
- changing position
- walking around – movement can encourage contractions
- a warm shower or bath
- a back rub
- a nap to regain your energy
- something to eat or drink
- options for pain relief – if you’re very tired or have pain.
-
What is the best position for giving birth?
Kneeling, on the bed or floor, leaning against a large pile of pillows, or supported by a partner. Some women may feel more comfortable with one knee up.

Squatting, supported by partner behind, or holding onto a bar. The woman should stand to rest between contractions. This may not be appropriate for women who have had epidurals.

Sitting, such as on a toilet or birth stool, with the legs wide apart and leaning forwards with the arms supported on the thighs, or by a partner.

-
What is an episiotomy?
An episiotomy is a surgical cut in the woman’s perineum (area between the vagina and anus) during birth.
You may need an episiotomy (with your consent) when for some reason, related to your baby or you, your doctor or midwife believes there is a chance that your perineum may tear when the baby’s head comes through during the second stage of labour. This is more likely to occur when forceps or a vacuum assistance is required.
Research has shown that the selective use of episiotomy may reduce a more severe vaginal or perineal tear.
-
How will my baby be monitored during labour?
During labour, your baby's heart rate will be checked regularly.
If you have had a healthy pregnancy and there are no problems at the onset of labour, your baby's heart will be listened to every 15 to 30 minutes using a small hand-held Doppler ultrasound device. This equipment can be used regardless of the position you are in, even in the shower.
If you had problems during pregnancy or if problems arise during your labour, your baby’s heart rate may be monitored continuously using a cardiotocograph (CTG).
More information: Queensland Clinical Guidelines parent information – Fetal monitoring in labour
-
What is a CTG?
A CTG (cardiotocograph) involves having two plastic disks (receivers) strapped to your abdomen and held in place by two belts. The receivers are attached to a machine, which may limit your movement. Some machines are wireless, enabling you to move around freely while you are being monitored. This is known as telemetry.
-
Why do I need internal (vaginal) examinations?
What happens during a vaginal examination?
When a woman's cervix thins during labour it is referred to as effacing. When her cervix is opening it is called dilating.
These cervical changes can be measured by the caregiver doing a vaginal examination with their gloved fingers during labour, often referred to as a VE.
During labour, vaginal examinations are usually carried out after a contraction finishes and when the woman says she is ready.
-
Can I take my placenta home?
Request to take the placenta home
The birth placenta holds significant value in some cultures and for some people. It is not uncommon for people to bring their baby’s placenta home, bury it in the garden and plant a tree above it.
You have the right to take your placenta home – speak to your midwife about the policy and how the hospital will support you.
-
How do I register my baby’s birth?
After baby is born, you will be given a birth registration pack.
Information includes:
- how to register your baby’s birth
- how to order a birth certificate/extract or commemorative birth certificate.
In the case of same sex female parents, only one parent can be registered as the baby's mother.
More information:
Next section: When complications occur
-
When complications occur
-
Plans may change
Every woman is different. Every labour is different.
Sometimes pregnancy, labour and birth may not go as planned. The reasons are usually complex.
This module will discuss the following important topics:
- pre-eclampsia
- preterm birth
- multiple birth
- breech
- overdue pregnancy
- monitoring in labour.
- concerns for baby in labour
- antibiotics during labour
- blood loss after birth
Always talk to your doctor or midwife if you are concerned.
-
Pre-eclampsia
Symptoms of pre-eclampsia may include:
- high blood pressure and the presence of protein in the urine
- severe headaches
- sudden swelling, weight gain
- blurred vision or seeing ‘stars’ or ‘spots’
- a sense of feeling very unwell.
What is pre-eclampsia?
Pre-eclampsia is a serious disorder of pregnancy characterised by high blood pressure and serious complications of other organs in the body. Without treatment, seizures can develop. This can be fatal for mother and baby.
It is the most serious medical complication of pregnancy, affecting around five to 10% of all pregnancies in Australia. Researchers still do not know exactly why it happens in some pregnancies.
Regular antenatal checks are vital to keep a check on your blood pressure. Sometimes medication is needed. The onset of pre-eclampsia can be fast! If you experience any of the symptoms, seek medical assistance urgently.
More information: Pregnancy, Birth and Baby – Pre-eclampsia
-
Preterm birth
What is a preterm (premature) birth?
A preterm birth is one that happens before 37 weeks of pregnancy. In about half of all preterm births, the cause is unknown.
Factors that increase the likelihood of a premature birth can be:
- a previous premature birth
- some conditions of the uterus or cervix, such as fibroids or a weakened cervix
- a multiple pregnancy
- a maternal infection
- some maternal medical conditions such as pre-eclampsia.
If babies are premature, they are likely to need extra care at birth.
More information: Queensland Clinical Guidelines parent information – Preterm labour and birth
-
Breech
A breech position means the baby presents bottom or feet first, rather than head first.
During pregnancy, many babies are in the breech position. However, most babies turn before 37 weeks.
If your baby is still breech at 37 weeks, the chances of your baby turning by itself are low.
Your doctor or midwife will discuss the implications of this for your birth plan and what options are available.
Your options may include:
- external cephalic version
- vaginal breech birth
- elective caesarean birth (usually performed after 39 weeks).
Breech vaginal birth
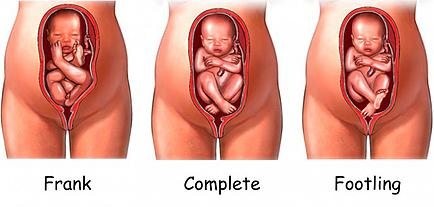
You may be suitable for a vaginal breech birth if:
- you go into spontaneous labour
- the estimated weight of your baby is within normal limits
- your baby is in either a complete (flexed) or frank (extended) breech presentation
- an ultrasound scan confirms your baby’s head is not extended
- the size and shape or your pelvis are adequate
- you have no pre-existing complications in your pregnancy.
Types of breech presentations
More information: The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) – Breech presentation at the end of your pregnancy
External cephalic version (ECV) for breech presentation
ECV is a commonly practiced procedure with a low risk of complications.
ECV can reduce the need for a caesarean birth. The success rate is approximately 40% for first time mothers and 60% for others. If you choose to have an ECV, the procedure is done in hospital.
- A trained doctor gently turns the baby by placing their hands on your abdomen and gently coaxing the baby around so it can be born head first.
- This procedure is done at around 37 weeks, using ultrasound to help see the baby, cord and placenta.
What you need to know
Mother and baby are monitored during the procedure.
There’s a small risk that turning the baby may tangle the cord or separate the placenta from the uterus – in which case an emergency caesarean birth is needed. If the baby is still in the breech position at the end of pregnancy, a caesarean birth may be recommended.
More information:
- Pregnancy, Birth and Baby – External cephalic version (ECV)
- The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) – Breech presentation at the end of your pregnancy
-
What if my pregnancy is ‘overdue’?
Note: treat ‘home remedies’ with a dose of caution.
A simple internet search will give you countless results for ‘natural’ ways to trigger labour. Be sure to get your midwife or doctor’s OK before trying any home remedies, herbal supplements or alternative treatments.
Around 80% of babies are born between 38 and 42 weeks of pregnancy. This is often called ‘at term’. Babies born after 40 weeks are described as ‘post term’.
It's OK to feel frustrated or disappointed if your pregnancy has gone past its due date. Try not to worry, soon you'll hold your baby in your arms and the long wait will be over.
While you are waiting, stay in touch with your midwife or doctor. You'll need frequent check-ups until your baby is born.
Take advantage of the extra time. You may want to:
- get some extra sleep
- make any final preparations for baby
- stock your freezer with meals
- review your birth preferences.
Overdue pregnancy
If your labour hasn’t started by 41 weeks, your midwife or doctor will probably offer you a 'membrane sweep’.
What is a membrane sweep?
A membrane sweep involves a vaginal (internal) examination that stimulates the cervix (neck of your womb) to produce hormones that may trigger natural labour.
If your labour still doesn’t start naturally after this, your midwife or doctor will discuss with you a date to have your labour induced.
If your pregnancy lasts longer than 42 weeks there is a higher risk of complications.
Your doctor or midwife will probably recommend regular tests to check on your health and your baby’s health. After 42 weeks, there is a higher risk of stillbirth or fetal compromise.
These tests might include an ultrasound to check the amniotic fluid index and an ultrasound to check the biophysical profile.
More information: Pregnancy, Birth and Baby – Overdue
-
How will my baby’s heart rate be monitored during my labour?
Intermittent monitoring
If you have had a healthy pregnancy and there are no problems at the onset of labour, your midwife will listen to your baby's heart beat every 15 to 30 minutes using a small hand-held Doppler ultrasound device.
Continuous electronic monitoring
If you or your baby have any known risk factors, continuous monitoring may be recommended.
This is done using a CTG (cardiotocograph) machine. This type of monitoring is external (outside your abdomen).
Telemetry
Telemetry is a wireless system of monitoring that can be used while you are mobile and walking around, even in the shower.
Fetal scalp electrode (FSE)
Sometimes it is necessary to attach the monitor directly onto your baby via a special lead. This is called a fetal scalp electrode. The lead is placed on your baby’s head during an internal vaginal examination. Telemetry (wireless) monitoring is still available using an FSE.
This type of monitoring is internal and is more reliable and accurate than external monitoring, particularly when you are mobile.
More information: Queensland Clinical Guidelines parent information – Fetal monitoring in labour
-
Concerns for baby in labour
When immediate birth is required
If there are concerns for baby’s wellbeing and immediate birth is required, baby will be birthed as soon as possible with vacuum or forceps (or perhaps by caesarean birth).
A change in the baby’s heartbeat can be a sign the baby isn’t getting enough oxygen. This is called ‘fetal distress’.
Signs of fetal distress include:
- a faster, slower or unusual pattern to the baby’s heartbeat
- a bowel movement by the baby seen as a greenish black fluid called ‘meconium’.
If these signs are present, your doctor or midwife will discuss with you, your continued management and care during your labour.
More information: Queensland Clinical Guidelines parent information – Fetal monitoring in labour
Why is meconium a concern?
Meconium aspiration syndrome
Meconium aspiration syndrome is when a baby inhales the meconium before, during or after labour.
It can cause respiratory problems as serious as pneumonia, and although it rarely happens, it can be fatal.
Meconium stained fluid occurs with about 10% of babies who are 'term' (37 to 42 weeks).
The presence of meconium during labour can be (but not always) a sign that the baby is becoming distressed.
Your labour will be observed closely and a paediatrician will be available at the birth, in case specialised care is required.
-
Antibiotic treatment during labour
Antibiotic treatment during labour may be recommended for:
- preterm labour – if you are in preterm labour, it may be caused by an infection
- PROM (Prolonged Rupture of Membranes) – to prevent a uterine infection
- Group B Strep infection
- having a fever during labour
- a preventative – in some situations, you may be given antibiotics as a preventative measure against potential infection, an example might be for a caesarean birth.
What is a Group B Strep (GBS) infection?
Approximately 15–25% of women are carriers of Group B Streptococcus, without any symptoms. Usually, you do not know you are a carrier.
It is usually detected by a vaginal swab. GBS can come and go during your pregnancy. If it is present when you give birth, there is a chance your baby can become infected.
If you are known to be GBS positive, and you have additional risk factors (e.g. your waters have broken and are therefore no longer providing a protective barrier for your baby), you will be offered antibiotics to try to prevent an infection in your baby.
More information: Queensland Clinical Guidelines parent information – Group B Streptococcus (GBS) in pregnancy
-
Blood loss after birth
Is it normal to bleed after birth?
Yes, bleeding in the days or weeks after birth (also called lochia) is completely normal and occurs regardless of whether you have a vaginal or caesarean birth.
How much bleeding is considered ‘normal’?
Women’s experiences of bleeding after birth vary considerably. In the first few days after birth, the majority of women experience moderate to heavy bleeding, however some experience minimal bleeding. This early bleeding is usually more red in colour.
Over the next few days to weeks, this bleeding will gradually decrease and will change colour. Women describe their blood loss to be browny-red, pinky-red, pale pink or a creamy colour.
The majority of women will stop bleeding between four and six weeks, however some women experience bleeding for longer than this. It is also common for bleeding to be heavier after breastfeeding.
More information: Queensland Clinical Guidelines parent information – Bleeding after birth
Abnormal blood loss
How much bleeding is too much?
- if you have a sudden and continued increase in your blood loss
- if the blood suddenly changes in colour to a brighter red
- if you are experiencing heavy blood loss and are feeling dizzy, weak, sweaty, pale, have a fast heartbeat or rapid pulse
- if your vaginal discharge is offensive (smelly) – this may indicate infection.
Every woman is different, however, as a general guide – if it has been more than 24 hours since birth and you are soaking more than one maxi-pad every two hours, you may be bleeding too much. If this is happening - call your doctor, midwife or 13HEALTH (13 43 25 84).
More information: Queensland Clinical Guidelines parent information – Bleeding after birth
Next section: Induction of labour and augmentation
-
Induction of labour and augmentation
-
Why are inductions needed?
Induction of labour (IOL) is a relatively common procedure.
The IOL rate in Queensland is about 22%.
IOL is a procedure used to stimulate contractions, before labour begins on its own. It includes the use of medication or other methods to bring on (induce) labour.
The reasons that an induction could be recommended include:
- your pregnancy is overdue
- multiple pregnancy
- your baby is small for their age
- your membranes have ruptured (waters have broken) and labour has not started
- certain medical conditions such as diabetes, high blood pressure or cholestasis.
Your doctor or midwife will discuss the reason for your induction at your antenatal visit.
More information: Queensland Clinical Guidelines parent information – Induction of labour
-
Frequently asked questions – inductions
What is a Bishop score?
It is a score used by doctors and midwives to determine how ‘ready’ your cervix is for labour. It is a combination of how soft, open and thin your cervix is, and where your baby is positioned in your pelvis. The score assists in deciding which method of induction will be most successful for you.
What is ‘cervical ripening’?
Ripening the cervix is a process that helps the cervix soften and thin out in preparation for labour. Medications or devices may be used to soften the cervix so it will stretch (dilate) for labour.
How will I be induced?
The method of induction will depend on:
- the condition of your baby
- your condition
- the progress of labour
- dilation of the cervix
- how far down in your pelvis the baby has gone
- the position of the baby's head
- your comfort and choice.
- Transcervical catheter ‘balloon catheter’.
- Prostaglandins, a ‘gel’ or pessary (Cervidil).
- Artificial Rupture of Membranes (ARM) ‘breaking your waters’.
- Syntocinon (oxytocin), sometimes called ‘the drip’.
What are some of the different methods of induction?
How long do inductions take?
There are lots of factors involved. Some women go into labour and deliver within a few hours after induction. Others take one or two days to start labour.
-
Questions to ask about induction of labour
Your midwife or doctor should discuss the pros and cons of any intervention so you can make an informed decision.
You should ask your doctor or midwife whether induction will:
- hurt?
- affect my recovery?
- affect my ability to breastfeed?
- affect any future pregnancies?
You should also ask questions such as:
- why would I need this intervention?
- what are the risks and benefits to me and my baby?
- are there any alternatives?
- is it likely to increase my need for more interventions?
- can I do anything while I’m pregnant to decrease my chances of needing the intervention?
- what is the hospital’s policy on this intervention and the evidence to support this?
More information:
- Queensland Clinical Guidelines parent information – Induction of labour
- Pregnancy, Birth and Baby – Induced labour
-
Methods of induction
Balloon catheter
A cervical ripening balloon catheter
This is a thin tube or catheter with balloons on the end. The catheter is inserted into your cervix and the balloons are inflated with saline (salty water).
Once inflated, the balloons apply pressure to the cervix. The pressure should soften and open your cervix.
What happens next will vary for each woman – some might need an Artificial Rupture of Membranes (ARM) to break their waters. Some women might need oxytocin to stimulate the contractions.
What do I need to know?
When the catheter is in place, you will need to stay in hospital, but you can move around normally. At about fifteen hours after the catheter has been inserted or when it falls out, you will be re-examined (vaginal examination).
More information: Queensland Clinical Guidelines parent information – Induction of labour
Prostaglandins (‘gel’)
What is a prostaglandin induction?
Prostaglandin is a hormone that prepares your body for labour. A synthetic version of this hormone is inserted into your vagina, behind your cervix, using a syringe (see image).
When the prostaglandin takes effect, your cervix will soften and open.
- you may need up to three doses (given every six to eight hours) over 12 to 24 hours
- some women may need an ARM to break their waters
- the gel may start your labour but you may still require other methods of induction, such as an ARM and/or a Syntocinon infusion.
What do I need to know?
A ‘gel’ induction can be a lengthy process, sometimes one to two days. If the process is started in the evening, you will need to rest while the gel is working. Your support person is advised to go home as there are no facilities to accommodate them overnight.
More information: Queensland Clinical Guidelines parent information – Induction of labour
Cervidil induction
What is Cervidil induction?
Cervidil is a tape that contains prostaglandin which is used to ripen (soften), shorten and open the cervix.
A vaginal examination is performed to assess the cervix and the tape is inserted behind the cervix.
- the end of the tape will be visible at the opening of the vagina similar to a tampon string
- your baby will be monitored by a CTG machine for a minimum of 20 minutes (monitors strapped to your abdomen)
- the Cervidil tape remains in for up to 24hrs
- this may cause backache or ‘period-like’ pains.
What do I need to know?
- once the induction process has started you will need to remain in hospital
- some women will react to the Cervidil and have nausea, vomiting or diarrhoea, or facial flushing (this is rare)
- the Cervidil may start your labour but you may still require other methods of induction, ARM and/or a Syntocinon infusion.
More information: Queensland Clinical Guidelines parent information – Induction of labour
Syntocinon (oxytocin) infusion
What is a Syntocinon induction?
Oxytocin is the hormone that causes contractions. A synthetic version (Syntocinon) can be given to start the induction process.
Syntocinon is given through a drip, usually in your hand or arm. Once contractions begin, the rate of the drip is adjusted so that contractions occur regularly until your baby is born.
This process can take several hours.
Your baby's heart rate will be monitored throughout labour using a CTG machine.
What do I need to know?
- you are attached to a drip and the CTG monitor which can affect your ability to move around during labour
- sometimes oxytocin can cause the uterus to contract too frequently, which may affect the pattern of your baby's heartbeat. If this happens, you may be asked to lie on your side and the drip will be slowed to reduce the number and strength of your contractions
the Syntocinon drip is only an option after your waters have broken.
More information: Queensland Clinical Guidelines parent information – Induction of labour
-
Risks of induction
- Your chance of needing extra pain relief is higher, because the contractions are often more painful.
- Your chance of having a caesarean birth is higher, if your labour is induced for a reason other than pregnancy lasting longer than 41 weeks, or it’s your first baby.
- Sometimes an induction doesn’t work in getting your body to go into labour (failed induction).
- As your baby’s heartbeat will be monitored with special equipment during your labour, it can be harder for you to move around and use the bath or shower for pain relief.
- Overstimulation of the uterus: this may require medications to reverse the effects of the over-stimulation or an emergency caesarean birth.
- Cord prolapse: this is extremely rare. When the waters are broken there is a very small risk of the umbilical cord slipping below the baby’s head with the fluid. This requires an immediate caesarean birth.
More information: Queensland Clinical Guidelines parent information – Induction of labour
-
Augmentation of labour
A labour that's progressing slowly can be augmented, which means certain techniques are used to speed it along.
If your cervix is opening slowly, or the contractions have slowed down or stopped, your midwife or doctor may suggest medications or techniques to speed up labour. This is known as augmentation of labour.
Methods include:
- amniotomy – breaking the waters or ‘ARM’
- oxytocin – this hormone is administered via an intravenous drip to stimulate uterine contractions.
It is important to note that both induction of labour and augmentation require extra fetal monitoring.
What else can I do if my labour is progressing slowly?
Your midwife may suggest changing your position, walking around, taking a warm shower or bath, or having a massage to encourage the contractions. If you’re tired or uncomfortable, you may want to ask about options for pain relief.
Next section: Assisted birth and caesarean birth
-
Assisted birth and caesarean birth
Medical interventions in labour
When are medical interventions needed?
A normal, problem-free labour is every pregnant woman's wish, however medical interventions are sometimes needed to help with the birth of a baby.
Some interventions include:
- forceps birth
- vacuum birth
- caesarean birth.
Why would I need an assisted birth?
Possible reasons for an assisted birth
Assisted vaginal birth accounts for around 11% of births in Australia. Reasons include:
For baby
- there are concerns about the baby's heart rate
- the baby is in an awkward position: facing up (occiput posterior ‘OP’ position) rather than facing down (occiput anterior ‘OA’ position).
For mother
- certain medical conditions, for example high blood pressure
- a prolonged pushing stage and maternal exhaustion.
-
Assisted birth – vacuum birth
Vacuum birth
This is the more common technique used for assisted deliveries. The vacuum cup is made of plastic and is attached to a suction device. A doctor inserts the cup into the vagina and creates a vacuum against the baby’s head. This helps the doctor to gently pull the baby out as you push.
What do I need to know?
- you may need an episiotomy
- if vacuum birth fails, a caesarean birth might be needed
- serious baby injuries after a vacuum birth are rare but can include bleeding under the scalp called a cephalhematoma
- it may cause a raised bruise on the baby’s head, but this soon fades
- minor scalp wounds from the pressure of the cup can occur.
More information: The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) – Assisted birth
-
Assisted birth – forceps birth
A doctor applies forceps, an instrument shaped like a pair of large spoons or ‘salad tongs’, to the baby's head to help guide the baby out of the birth canal. This is done during a contraction while you push.
Forceps birth and baby
What do I need to know?
- you may need an episiotomy
- if forceps birth fails, a caesarean birth might be needed.
Your baby may experience:
- minor marks on the face which are temporary
- minor facial injuries due to the pressure of the forceps
- temporary weakness in the facial muscles (facial palsy)
- minor external eye trauma.
Serious baby injuries after a forceps birth are rare but could include:
- skull fracture
- bleeding within the skull
- seizures.
More information:
- Queensland Clinical Guidelines parent information – Instrumental vaginal birth
- The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) – Assisted birth
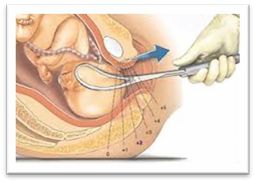

-
Caesarean birth
Around one in four Australian babies is birthed by caesarean section. A caesarean section is usually performed under regional (spinal or epidural) anaesthesia. However, sometimes general anaesthesia is required.
A caesarean section is a major surgical operation in which your baby is born through a cut in your abdomen and uterus.
Elective caesarean births are planned in advance because of existing problems with your pregnancy, or if you have had a previous caesarean.
Emergency caesarean births - usually the decision to perform an emergency caesarean is made during the course of labour. An emergency caesarean birth is recommended for the following reasons:
- there is concern for your baby’s wellbeing
- there is concern for your wellbeing
- there is a life-threatening emergency for you or your baby.
More information: Pregnancy, Birth and Baby – Caesarean
Elective caesarean birth
A planned or elective caesarean birth is required when there is a medical need for the operation. Medical reasons for having a planned caesarean birth include, but are not limited to:
- severe pre-eclampsia
- multiple births
- position of the baby – your baby may be in an abnormal position inside the uterus, making vaginal birth difficult
- placenta praevia – this is when the placenta blocks the exit to the uterus
- infection – if you have an active viral infection, such as genital herpes
- you have a medical condition – for example, a heart problem
- restricted growth of the baby
- previous caesarean birth.
More information:
- Raising Children Network – Your planned caesarean birth
- The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) – Caesarean section
Emergency caesarean birth
In an emergency, there may not be enough time to discuss the options of a caesarean birth. If vaginal birth poses significant risks to you or your baby’s health, a caesarean birth may be the safest option.
Reasons for needing an emergency caesarean birth include:
- Your baby cannot tolerate uterine contractions and gets distressed
- your labour is not progressing - despite your best efforts - causing distress to you and your baby
- your labour has been induced, but the methods used are failing to produce effective contractions
- you have vaginal bleeding during your labour
- an emergency where baby needs to be born very quickly and vaginal birth is not possible.
More information: Pregnancy, Birth and Baby – Emergency caesarean
-
What can I expect for a caesarean birth?
Before your surgery (if elective):
- you will need to meet an anaesthetist. This may be in a ‘pre-admission’ appointment at the hospital to talk about your anaesthetic for surgery
- you may be asked to take an antacid tablet, at home, the night before surgery
- you will need to fast from midnight, the night before the morning ‘list’ for elective surgery (or at another time specified)
- a small shave of the top part of the pubic area may be recommended, where the wound dressing will be applied after the surgery
- you will need to remove all jewellery, piercings and nail polish prior to surgery (toe nail polish may be acceptable but not fingernails).
On the day of your surgery (elective or emergency):
- you will be placed in a hospital gown, compression stockings and theatre cap
- a cannula will be inserted into your hand/arm (to give you intravenous medications)
- you will be given an epidural, if you have not already had one during labour
- once the epidural is working well, you will have a urinary catheter inserted into your bladder, as you will be unable to go to the toilet with an epidural in place
- you are usually in the operating theatre for an hour or more
- unless you are having a general anaesthetic, your partner can be with you in the operating theatre
- your partner will need to wear closed-in shoes, for workplace health and safety reasons
- you will have a midwife stay with you and look after you and your baby in theatre and afterwards in the recovery area
- unless you have had a general anaesthetic, skin to skin contact with your baby will occur very soon after birth
- the midwife will help you with feeding your baby.
Where will my baby go?
After your caesarean birth
- if you and your baby are both well, your baby will go with you to the postnatal ward and ‘room-in’
- if your baby is unwell, or needs to be monitored more closely, he/she may need to go to the Special Care Unit or Neonatal (newborn) Intensive Care Unit. Your partner may go with your baby until you are able to join them
- if your baby is unable to have skin to skin contact or breastfeed, you will be encouraged to express breast milk for your baby. Your midwife will assist you with this.
Caesarean birth recovery
How long will I be in hospital?
After your caesarean birth, you will stay in hospital for about three to five days.
A caesarean birth is major surgery, so your physical recovery is important. This is also a great time to get to know your new baby, with the support of hospital midwives and doctors.
Vaginal birth after caesarean (VBAC) is possible. After a previous caesarean birth, around 60–80% of women who attempt labour will have a vaginal birth.
More information:
- Queensland Clinical Guidelines parent information – Vaginal Birth After Caesarean (VBAC)
- Raising Children Network – Vaginal birth after caesarean (VBAC)
-
Risks of caesarean birth
Complications of a caesarean birth are rare but can include:
- Increased likelihood of blood loss. Depending on the degree of bleeding, some women may require a blood transfusion and/or hysterectomy (this is very rare).
- Risk of complications associated with having surgery, such as blood clots, scalpel cuts to the bladder or bowel (this is rare).
- Risk of a wound infection.
- Slower recovery time.
- Increased likelihood of complications in future pregnancies. For example, the placenta being low lying (placenta previa) or growing into the scar on the uterus (placenta accreta) which can lead to severe bleeding or further caesarean birth(s).
- Risk of baby having breathing problems and requiring admission to the Neonatal Intensive Care Unit or Special Care Nursery.
- Risk of scalpel cuts to the baby.
- Increased likelihood of the baby having feeding problems.
More information: Queensland Government – Caesarean Section Consent form
Next section: Pain relief options
-
Pain relief options
-
Managing pain in labour
Understanding the choices of pain relief are an important part of getting ready for the birth of your baby.
Although having a baby is a natural process, it can cause significant pain and discomfort.
Every woman is different, and every birth experience is unique, so the need for pain relief varies.
During labour, your need for pain relief may change, so it’s important that you are open to learning about different ways to manage pain during labour.
-
Transcutaneous electrical nerve stimulation (TENS)
Using a TENS machine in labour
- Electrodes are taped onto your back and connected by wires to a small battery-powered stimulator.
- With the stimulator, you give yourself small, safe amounts of current through the electrodes.
- You can move around while you use the TENS machine.
How do TENS machines help during labour pain?
TENS is believed to work by stimulating the body to produce more of its own natural painkillers, called endorphins.
- It reduces the number of pain signals that are sent to the brain by the spinal cord.
- TENS has been shown to be most effective if used during the early stages of labour when many women experience lower back pain.
- There are no known side effects for either you or the baby.
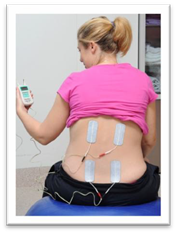
More information: Pregnancy, Birth and Baby – TENS (Transcutaneous electrical nerve stimulation)
-
Sterile water injections (SWIs)
How are SWIs given?
- the procedure involves a small amount of sterile water (0.01–0.02 mL) injected under the skin at four locations on the lower back (sacrum)
- the injections cause a brief but intense stinging sensation, that lasts for about 30 seconds and then wears off completely
- to distract from the stinging sensation, the injections are done during a contraction by two midwives.
How can SWIs help during labour?
During labour, SWIs provide effective pain relief for up to 85% of women with back pain and can last for up to two hours.
SWIs have a number of advantages, they:
- often have an immediate effect
- have no effect on the mother's state of consciousness
- have no effect on baby
- do not limit mobility
- do not adversely affect labour progress
- are a simple procedure that can be administered by your midwife and can be repeated as needed.

More information: Pregnancy, Birth and Baby – Non-medical pain relief during labour
-
Nitrous oxide (gas)
How do I use nitrous oxide in labour?
- you control the amount you use
- start breathing on it as soon as you feel a contraction coming on, so you will get the full effect when the pain is at its peak
- avoid use between contractions or for long periods as this can make you feel dizzy.
What is nitrous oxide?
Nitrous oxide is a gas that is mixed with oxygen and administered through a face mask or a mouthpiece held in the mouth.
Nitrous oxide is simple and quick to act and wears off in minutes. It will not take the pain away completely, but it may help.
More information: Pregnancy, Birth and Baby – Gas (Entonox)
-
Morphine
What are morphine injections?
Morphine is a strong pain reliever, usually injected directly your arm or thigh.
- the effect of morphine can last anywhere from two to four hours.
- morphine can make you feel sick, so anti-nausea medications are usually administered at the same time.
What are the possible side effects?
For mother:
- dizziness and nausea
- disorientation and altered perception
- respiratory depression (reduced breathing).
For baby:
- because baby is exposed to the drug via the umbilical cord, it may cause difficulty with breathing at birth, particularly if the baby delivers soon after a morphine injection
- it may also interfere with breastfeeding.
-
Epidurals
Why are epidurals used during labour and birth?
Epidurals are used for vaginal and caesarean births, because they allow the mother to stay awake and alert during the baby’s birth.
What are the advantages of an epidural?
- epidurals are usually a very effective form of pain relief
- epidurals take away the pain of contractions
- epidurals can be effective for hours and can be increased in strength if you need to have an emergency caesarean birth
- in a long labour, an epidural can allow you to sleep during the active stage of labour, saving energy in preparation for pushing in second stage of labour
- if your blood pressure is high, an epidural might be recommended by your doctor.
More information:
What happens when I have an epidural?
Epidural is a local anaesthetic, which is injected into your back (not the spinal cord).
An anaesthetist will put the epidural in. This usually takes about 20 minutes.
- a drip will be put in your hand or arm
- to place the epidural, you will be asked to either sit up or lie on your side
- cold antiseptic solution will be painted onto your lower back to clean the skin
- local anaesthetic will be injected into your back first – this may cause a stinging sensation for a few seconds
- you will feel a pushing sensation in your back while the epidural is inserted
- it is very important that you keep still while the epidural is inserted, to avoid any damage to the nerves in your spine
- the epidural needle is not left in the back - just a thin tube (called an epidural catheter) remains to deliver the epidural medications.

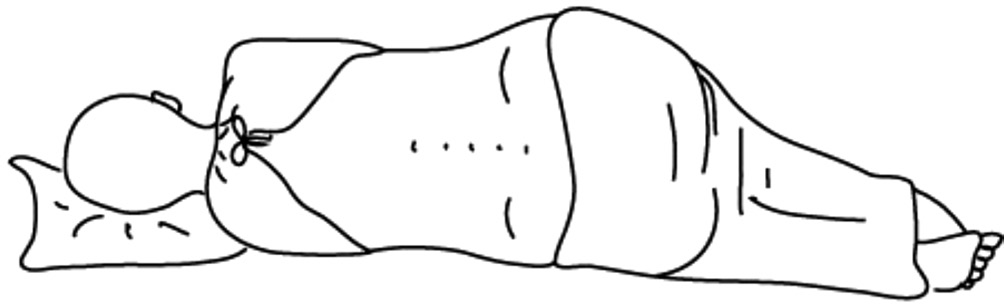
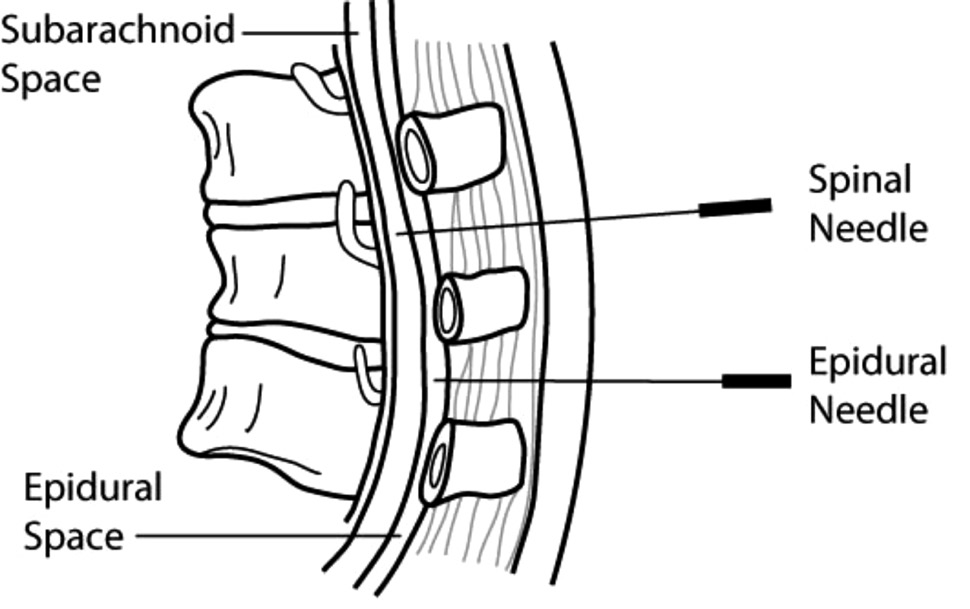
What can I expect for an epidural?
An epidural causes muscle weakness in the legs, so women who have had an epidural in labour are confined to bed.
This also means:
- an epidural can take away the sensation to pass urine so you will need a urinary catheter (a thin tube) to drain your urine
- you will have an IV (intravenous) drip in your hand to give you extra fluids
- a cardiotocography (CTG) machine will continuously monitor the baby’s heartbeat
- your blood pressure will be monitored closely
- in second stage of labour, you may still feel the urge to push, but the sensation is reduced so you may require an assisted delivery for your birth.
Frequently asked questions – epidurals in labour
Will an epidural hurt?
The answer depends on who you ask. Some women describe an epidural placement as creating a bit of discomfort in the area where the back was numbed, and a feeling of pressure as the small tube or catheter was placed.
When might an epidural not be recommended for pain relief?
There are certain situations where an epidural would not be recommended. For example, medical complications, bleeding disorders, infections, history of back surgery.
Discuss any concerns you may have with your midwife or doctor who will make a referral for you to speak to an anaesthetist prior to your birth.
When can I have an epidural?
Typically, epidurals are placed when the cervix is dilated to 4–5 centimetres or more and you are in true active labour. The timing is determined by your unique experience in labour. You will need to discuss this with your midwife or doctor at the time.
Can an epidural slow down my labour?
Yes. An epidural can cause your labour to slow down and make your contractions weaker. If this occurs, you may be given intravenous oxytocin to help speed up labour. The second stage of labour can be prolonged and assisted birth may be required in certain situations.
Can an epidural affect my baby?
Research shows that epidurals do not directly affect your baby. The drugs used in epidurals do cross the placenta but are considered safe and have minimal effect on baby.
What are the risks of an epidural?
Epidurals have been routinely used for many years and are widely accepted as an effective method of pain relief after surgery, during labour and childbirth. However, as with many medical procedures, there are some associated risks that, although small, you should be aware of before deciding whether to have an epidural.
Risks and benefits of epidurals: Queensland Government – Epidural pain relief for your labour
More information: Pregnancy, Birth and Baby – Epidural
Next section: Breastfeeding 101
-
Breastfeeding
-
Breastfeeding 101
Why breast milk?
Perfect food
Breastfeeding is the natural, biological way of providing babies with nutrients required for healthy growth and development.
Better for mum, better for baby
Breastfeeding helps with mother and baby emotional attachment and is better for both short and long term health.
Environmentally friendly
Breast milk has no waste products, so it is better for the environment.
Risks of not breastfeeding
For mothers
Higher risk of:
- ovarian cancer
- breast cancer
- type 2 diabetes.
More expensive:
- cost of formula
- cost of healthcare for a sick baby.
For babies
Higher risk of:
- gastrointestinal infections
- chest infections
- ear infections
- childhood leukaemia
- SIDS (sudden infant death syndrome)
- some long term diseases, for example diabetes
- allergies and milk intolerances.
For the community
- higher healthcare costs
- using up natural resources
- higher waste products in the environment.
Babies know how to breastfeed
Babies know when they are hungry and thirsty. Babies know when the milk comes in. Babies know how to breastfeed.
Allowing babies to do what they were born to do, will make for a much smoother transition into this new world; for mother and baby.
More information:
- Queensland Clinical Guidelines parent information – Breastfeeding your baby
- Breastfeeding information in other languages:
- Breastfeeding and postnatal care, Victorian Government
- Breastfeeding your baby, Royal Women's Hospital, Victoria
- Breastfeeding resources in other languages, Australian Breastfeeding Association
- Global Health Media – Breastfeeding videos in other languages
- Queensland Health – Breastfeeding information for Aboriginal & Torres Strait Islander people
What are the recommendations?
The World Health Organization and the National Health and Medical Research Council (NHMRC) recommend you breastfeed your baby exclusively for the first six months. Breast milk is all the food and drink that a baby needs.
The Australian Dietary Guidelines (NHMRC) recommends:
- breastfeeding as the best method of feeding full-term babies
- exclusive breastfeeding for around six months of life
- breastfeeding continues beyond six months while appropriate solid foods are introduced
- along with solids, women are advised to continue breastfeeding until 12 months of age, for as long as the mother and child decide.
Baby-friendly Hospital Initiative
The Baby-friendly Hospital Initiative (BFHI) was developed by the World Health Organisation and UNICEF in 1991. It is a worldwide program aiming to create a healthcare environment that supports mothers and babies to have the best start in life.
Queensland Health is proud to support the BFHI. We promote breastfeeding as the optimal way to feed your baby; however we also respect how you choose to feed your baby.
-
In pregnancy – planning for breastfeeding
Think about what is important for you.
It is never too early to read, learn and talk about breastfeeding.
Most people have a view about breastfeeding before having their baby. What have you heard from friends, television, or in the community?
Pregnancy – breast changes
Learning about the changes in your breasts during pregnancy may give you a better understanding of your body’s ability to breastfeed. The good news is, no physical preparation is required!
Most women notice breast changes in pregnancy, however some do not. Your breasts will usually increase in size – as the due date approaches, hormone changes cause your breasts to feel larger and tender. Sometimes, visible veins appear. In the third trimester, some pregnant women begin to leak colostrum from their breasts.
How your body makes milk
Your breasts are filled with milk making glands that are called alveoli. This is where your milk is produced. The milk travels from the alveoli through a series of milk ducts to the nipple openings.
The more often your baby breastfeeds, the more milk your breasts make.
Breastfeeding hormones
When your baby breastfeeds, your brain releases two hormones.
Prolactin is the hormone that causes your breasts to make milk.
Oxytocin helps with your letdown reflex (release of milk). These hormones also increase the level of bonding and comfort you feel during breastfeeding.
What happens during milk let down?
When your baby latches on and begins to breastfeed, the alveoli release milk. This is called the let down or milk ejection reflex. Let down occurs several times during a feed. In the early days, you may not even notice this is happening.
How can I tell if my milk is letting down?
- sensation of warmth or tingling in the breast
- sudden thirst
- milk dripping from the other breast
- ‘after birth’ pains
- changes in the baby’s sucking pattern from quicker sucks to slower deeper sucks.
More information: Australian Breastfeeding Association – Breastfeeding Information
Can all mothers breastfeed?
Most women can breastfeed with the right information, support and practice.
Speak to your midwife, doctor or lactation consultant if any of the following applies to you:
- previous breast surgery
- a medical condition requiring medications
- diabetes
- your current pregnancy is twins (triplets, quads, etc).
More information: Australian Breastfeeding Association
Things to think about while you are pregnant
- Why have you decided to breastfeed your baby?
- What information about breastfeeding do you already have?
- Are family members supportive of your interest in breastfeeding?
- Will someone be at home to help you in the early weeks?
- Do you have any special medical problems that require treatment or medications?
- Have you ever had breast surgery? What was the reason?
- How long do you plan to breastfeed?
- Do you plan to return to work/school/study after your baby is born?
- If you have breastfed other children:
- How long did you breastfeed?
- Why did you stop?
- Did you have any problems?
-
Breastfeeding – the first few days
The first feed
Most babies will attach to the breast for their first feed if placed skin to skin (in contact) with their mother.
Skin to skin contact
This is when your baby is placed directly from birth onto your chest or abdomen. Your newborn’s skin touches your skin. A blanket or towel can be placed over the baby’s back for warmth if required. Providing baby and you are well, skin to skin contact should continue, undisturbed, until the first breastfeed. Routine procedures such as bathing and weighing can wait.
If you can’t have skin to skin right after the birth, this is often due to medical reasons.
Your midwife will support skin to skin contact as soon as possible.
More information: Queensland Clinical Guidelines parent information – Breastfeeding your baby

Most healthy babies will want to feed within the first 90 minutes after birth.
During skin to skin contact, your baby will show feeding signs (cues).
When this happens, position baby close to your breast.
Bonding and rooming in
After your baby is born, you will both be in the same room – you will be able to see signs that your baby is hungry, uncomfortable or needs to be cuddled.
Benefits of rooming in:
- babies cry less and are easier to calm
- mums get more rest
- you can respond to baby's early feeding cues and feed on demand
- you will make more breast milk when you feed your baby often.
The first few days
Newborn feeding behaviour
Birth to two hours
Baby is usually awake and alert (best time to feed).
The first 24 hours
Two to 20 hours after birth, baby will have light and deep sleep (may not want to feed often).
After 20 hours
Baby will have sleep and awake behaviour (and may want to feed often).
Day two to three
Your baby may seem unsettled on day two or three while your colostrum changes to mature milk. Increased breastfeeding is often all that is needed.
More information: NHS – Breastfeeding: the first few days
-
Signs of hunger
Mothers can follow their baby's lead in how often to breastfeed.
Rather than watching the clock, watch for cues that your baby is hungry such as the rooting reflex, chewing/sucking on hands or fingers.
Early feeding cues (signs) are the best time to feed!
Early cues: “I’m hungry” (stirring, mouth opening, turning head and seeking/rooting).
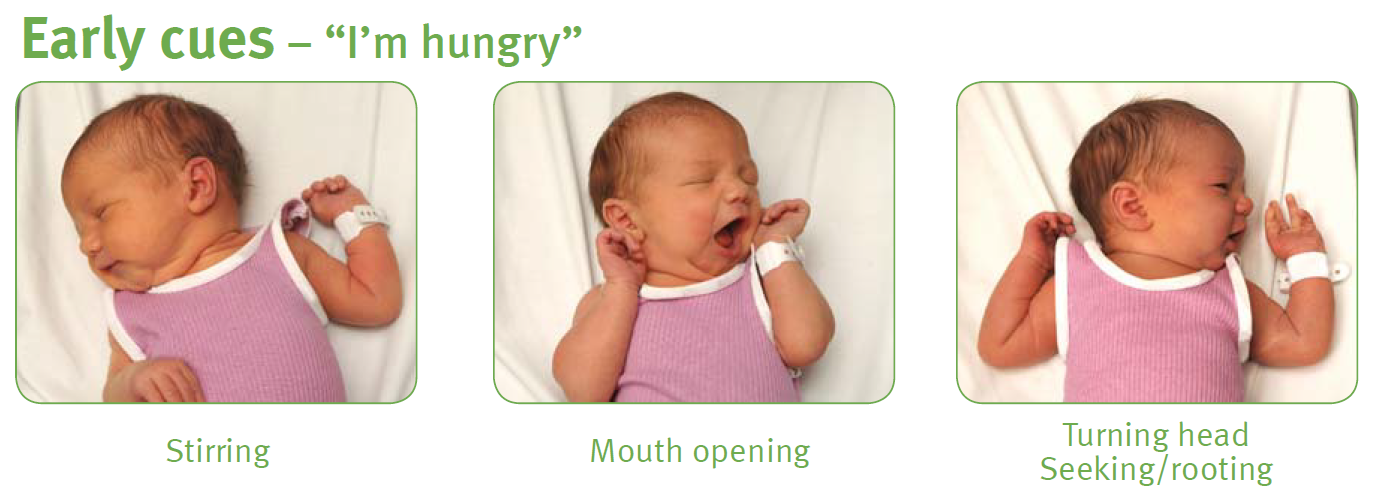
Mid-cues: “I’m really hungry” (stretching, increasing physical movement, hand to mouth).

Late cues: “Calm me, then feed me” (crying, agitated body movements, colour turning red).
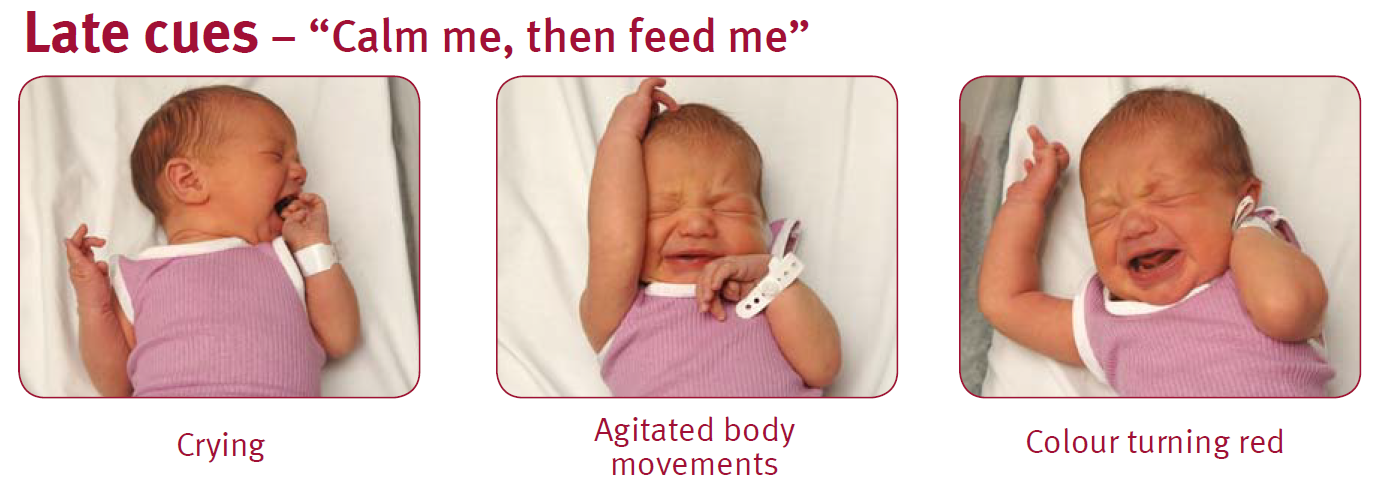
-
Breastfeeding – the early weeks
How your milk changes
The first milk is called colostrum. This special milk is yellow in colour, thick and sticky. It may be low in volume but it is high in concentrated nutrition for your newborn.
Colostrum has a laxative effect on baby, helping him or her pass the early stools and helping to prevent jaundice.
The more you feed your baby, the more milk you will make (supply = demand).
Days after birth
Type of milk
How it looks
Birth to day 2 or 3
Colostrum
Thick, yellow in colour, small amount
Days 3 to 5
Transitional milk
Mixture of colostrum and mature milk more plentiful
Days 5 to 7
Mature milk begins
Thinner, whitish, plentiful
When does milk ‘come in’?
You may find that your breasts become larger and feel heavy, warmer and uncomfortable when your milk ‘comes in’; usually about two to four days after your baby is born.
Your milk will then increase in volume and will generally begin to appear thinner and whiter in colour.
How often will baby feed?
Whenever baby is hungry!
Healthy, full-term newborns should breastfeed eight to 12 times in each 24 hour period. Many mothers are surprised at how quickly and easily human milk is digested, often within 90 minutes of the last feed.
Many babies do what is called 'cluster feeding’, spacing feeds closer together at certain times of the day (usually during the evening). This is normal. As babies grow and their stomachs become larger, they begin to go longer between feeds and develop more regular feeding patterns.
How long does a feed take?
Your baby will determine this.
A typical feed might last about 20–30 minutes. In the beginning, it could take up to an hour.
It is important that you allow the baby to feed for as long as the baby wants on one side.
Do not time the feed or swap sides unless the baby seems to have finished one side. This will ensure that your baby feeds well and helps with your breast milk supply.
If the baby takes only one breast, remember to offer the other breast at the next feed.
When your baby has had enough, they will stop sucking and come off the breast or simply fall asleep. If you notice that baby's jaw isn't moving anymore, you can detach baby. Your breasts keep making milk.
Remember, supply = demand.
How to tell if your baby is getting enough milk
A common concern to breastfeeding mothers is how to tell whether their baby is getting enough milk.
Your baby will tell you by:
- being content between most feeds
- having six to eight wet nappies a day, by seven days of age
- their poo changing in colour, from black meconium stool to soft yellow by seven days of age
- starting to put on weight. Many babies may lose up to 7% of their birth weight during their first days of life. Babies usually regain the weight by two weeks of age.
Seek advice from a healthcare professional if you have concerns.
Age
Feeds per day
Wet nappies
Dirty nappies
Day 1
3–8
1
1
Black, tarry and sticky
Day 2
5–10
2–3, may contain urates.
What are urates? Crystals present in strong urine that stain a nappy reddish-orange.
1–2
Greenish–black, softening
Day 3
5–10
3–4 paler, but may be concentrated and contain urates.
3–4
Greenish–yellow, soft
Day 4
5–-10
4–6 pale, no urates.
4 large or 10 small
Yellow and/or seedy, soft/liquid
Day 5
8–12
More than 6 pale nappies.
4 large or 10 small
Yellow and/or seedy, soft/liquid
-
Positioning and attachment
The key to successful breastfeeding is comfortable positioning and good attachment.
Make sure your baby is well attached to the breast. If your baby is only attached to the nipple, breastfeeding will be painful.
If your baby is well-attached to your breast, you are less likely to experience breastfeeding problems like cracked nipples, and your baby will get the most amount of milk from your breast.
Find a comfortable place where you can sit and relax. Have everything you might need close to hand – e.g. phone, glass of water. Breastfeeding may take some time.
Positioning and attachment
This webpage is currently being reviewed and some outdated content has been removed. Please refer to Raising Children Breastfeeding videos and Raising Children Breastfeeding positions in pictures in the interim.
Some tips which may help:
- Make sure you are comfortable and well supported. Lean back rather than sit upright. Place your baby on your bare chest between your breasts, facing you. Gravity will help keep your baby in position.
- When calm, your baby will begin to follow their instincts. Your baby will start to move towards one breast. Support your baby behind their shoulders and under their bottom (avoid holding their head). Let your baby move towards your nipple – they know where to go!
- Your baby will most likely position themselves on an angle, with mouth near your nipple and feet supported by your thigh or lap.
- When your baby is just below your nipple, they will dig their chin into your breast, reach up with an open mouth and attach to the breast.
- When your baby is feeding well, they will suck deeply and regularly (sometimes with short pauses), and you’ll hear swallowing.
More information: Raising Children Network – Breastfeeding positions: in pictures
-
Signs of an effective attachment
How to tell if your baby is attached:
- you are comfortable
- baby looks comfortable, relaxed and not tense, frowning or wriggling
- baby’s mouth is open wide against the breast with nipple and breast in mouth
- baby’s chin is touching the breast
- cheeks not sucked in
- baby has deep jaw movement with drinking
- swallowing can be seen and possibly heard once the milk “lets down”
- after feeding, nipples may appear slightly longer but are not flattened, white or pinched.
Video: Raising Children Network – Breastfeeding: getting a good attachment
How to tell if your baby is not attached
Your baby is not attached if:
- baby’s mouth is not open wide
- baby’s lips are curled inwards
- baby has only the nipple or a small amount of breast in the mouth
- you hear a clicking sound when baby is sucking
- you do not hear or see swallowing
- you feel pain when breastfeeding.
Breaking the attachment
Avoid pulling your baby away from your breast. Instead, break the attachment by inserting your little finger into the corner of your baby’s mouth, between the gums, and gently remove your baby from the breast.


-
Breastfeeding positions
Front hold or cradle

Underarm or football hold

Side lying

Video: Raising Children Network – How to breastfeed: breastfeeding positions
More information: Australian Breastfeeding Association – Attachment to the breast
-
Common breastfeeding questions and concerns
Newborn jaundice
Why is my baby’s skin yellow?
Jaundice in the first week of life occurs in 60% of healthy newborn infants. It typically occurs between day two to four after birth and is usually cleared by the first week.
Frequent feeding is the best prevention. If a baby appears to be jaundiced, a blood test can determine the level of bilirubin. Treatment, if any, will depend on the level of bilirubin, how the baby is feeding and how old the baby is. Jaundice appears first on the face and head. If the level of bilirubin goes higher, it will appear on the body, and if it goes even higher it will be on the palms of the hands and soles of the feet.
More information: Queensland Clinical Guidelines parent information – Jaundice in newborn babies
Using a dummy
If you’re breastfeeding, it’s a good idea to avoid using a dummy until breastfeeding is established. This is usually when your baby is four to six weeks old.
Using a dummy (also known as a pacifier) when you plan to breastfeed can:
- lead you to miss those early cues that your baby is ready to feed, thus delaying your milk coming in
- decrease the amount of times you feed your baby
- contribute to low breast milk supply and/or engorgement
- be a factor in low weight gain for baby
- increase baby’s risk of ear and thrush infection
- contribute to an earlier return of your fertility.
More information: Queensland Clinical Guidelines parent information – Breastfeeding your baby
Partners: how can I support my partner?
Partners of new mothers play an important role, they can:
- provide emotional support
- help calm a fussy baby
- bring the new mother food and drink while she is breastfeeding
- reassure the mother that breastfeeding is one of the most important things to give your baby the healthiest start to life
- deflect any negative comments from friends or relatives
- tell her she is doing a great job!
More information:
- Raising Children Network – New dads: 10 tips for making a great start to fatherhood
- Raising Children Network – Grandparents and kinship carers
Video: ACT Government Health – Breastfeeding Give it a Go
Healthy nutrition for breastfeeding mothers
Healthy eating is important when you are breastfeeding.
Your body has a greater need for most nutrients; to meet these needs it is important to eat a healthy, well-balanced diet based on a range of healthy foods and plenty of water.
More information: Queensland Health – Nutrition Education Materials Online (NEMO)
Recommendations about smoking, drinking alcohol and caffeine
Smoking is not recommended while breastfeeding.
Smoking can affect the nutrient content of breastmilk and reduce supply. It also increases the risk of SIDS (sudden infant death syndrome).
Avoid exposing baby to tobacco smoke. Don't let anyone smoke near your baby – whether in the house, car or anywhere else your baby spends time.
For advice and support visit QUIT HQ or call Quitline on 13 78 48.
Alcohol
The safest option is to avoid drinking alcohol while breastfeeding.
Caffeine
Breastfeeding mothers can safely consume caffeine, but they should consume less caffeine than non-breastfeeding women, to protect their health and the health of their breastfed baby.
Medications and breastfeeding
If you have an existing medical condition or are taking an over-the-counter or prescribed medication, discuss this with your health professional.
Always discuss alternative/natural and complementary therapies, as they may not be safe during breastfeeding.
Always check with your doctor or pharmacist regarding prescription and over-the-counter medications when you are breastfeeding.
More information: Australian Breastfeeding Association – Common concerns - baby
-
Common breastfeeding issues
Many women experience some difficulties when establishing breastfeeding.
Most are minor and can be overcome by advice, assistance and support.
Your midwife or a lactation consultant will be happy to help.
For advice contact:
- 13 HEALTH (13 43 25 84)
- Australian Breastfeeding Association Breastfeeding Helpline: 1800 mum 2 mum (1800 686 268)
Engorgement
About three days after having a baby, many mothers will experience breast fullness as their milk 'comes in'. Occasionally a mother may need to express a small amount of milk to soften the breast before a feed. This fullness usually only lasts for 24 hours and is different to engorgement.
Signs of engorgement
- breasts full and painful, with swelling down to areola of breast
- baby may be unable to attach to breast because of fullness.
- limiting the time baby feeds at the breast
- using dummies to extend time between breastfeeds
- baby not being properly attached to the breast.
- massage and warm packs to breast prior to the feed
- express a small amount of milk before feeds to make breasts softer for baby to attach
- feed your baby frequently
- apply cold packs on breast between feeds
- avoid wearing a tight bra
- if symptoms continue, or worsen, seek assistance.
What causes engorgement?
- limiting the time baby feeds at the breast
- using dummies to extend time between breastfeeds
- baby not being properly attached to the breast.
How to treat engorgement
- massage and warm packs to breast prior to the feed
- express a small amount of milk before feeds to make breasts softer for baby to attach
- feed your baby frequently
- apply cold packs on breast between feeds
- avoid wearing a tight bra
- if symptoms continue, or worsen, seek assistance.
Concerns with milk supply
Building your milk supply
When it comes to breastfeeding, remember that supply equals demand. The more you feed your baby, the more milk your breasts will make.
Ways to increase or maintain a good milk supply include:
- respond to your baby’s feeding cues both day and night
- avoid giving any extra feeds from bottles – this reduces your baby’s need to suck at your breast and reduces your milk supply
- avoid the use of dummies until breastfeeding is established (four to six weeks)
- express milk in between feeds to increase your supply.
Sore, damaged nipples
Nipples can be sensitive in the beginning, but breastfeeding should not be painful through a whole feed or continue to be painful.
Helpful hints to avoid sore nipples:
- make sure your baby is well attached to the breast, not just to the nipple
- apply small amounts of expressed breast milk on the nipple after feeding and allow to dry
- replace damp breast pads frequently
- try different feeding positions
- if breastfeeding continues to hurt, or there is nipple damage, seek help.
Cracked/bleeding nipples:
- make sure baby is attached well
- apply small amounts of expressed breast milk on the nipple after feeding
- if there is a need to rest breasts, you should express breastmilk to keep up supply.
If your nipples are cracked or bleeding it is recommended that you seek help from a health care provider.
Mastitis
Mastitis is an inflammation and/or infection of the breast tissue.
Mastitis can be caused by:
- a blocked milk duct or nipple damage
- milk oversupply that is ongoing
- baby not being attached well to the breast
- mother’s stress, fatigue or poor nutrition.
Signs of mastitis
- an area on the breast that is red and swollen
- breast feels hot
- skin on breast may look tight, shiny and red
- mother feels very unwell with flu type symptoms and a temperature greater than 38.5oC – if so, seek medical help immediately.
Management of mastitis
- seek treatment from a doctor immediately – antibiotics should be started
- continue to breastfeed or express to avoid complications
- keep feeding on the side that is not infected and also offer the infected breast (the milk from the affected breast is safe for baby)
- get plenty of rest and drink plenty of fluids.
More information:
- Australian Breastfeeding Association – Common concerns - mum
- Queensland Health – Queensland Milk Bank
Next section: Expressing and storing breastmilk
-
Breastfeeding in the first year
Looking after yourself
Practical support
Involve your family and friends who can provide a network of help with babysitting, social activities and ‘time out’ for you.
Personal support
Talk to friends, family and support groups about how you are feeling.
Information support
Seek information from health professionals, books, websites etc. It can be challenging for you to identify what information is based on the latest recommendations, so be wary of the source of information.
Ways to take care of yourself
- sleep when your baby is sleeping
- limit outside activities and visitors in the early weeks
- drink water when you are thirsty and eat healthy foods
- try to get exercise and fresh air every day
- join a breastfeeding or new mother support group
- talk about your feelings with your partner or others
- let family and friends help with chores
- take as much time off work as practically possible.
Family planning
The return of the menstrual cycle is different for every woman.
Even if you are exclusively breastfeeding, you can start ovulating. That means you can get pregnant again without even knowing that it has happened.
Ask your healthcare professional about your family planning options and if they are compatible with breastfeeding.
Work and breastfeeding
The Australian Breastfeeding Association has useful information on breastfeeding and work.
Newborn sleep and settling
Crying is an important means of communication for young babies. Babies always cry for a reason. These include:
- tiredness
- hunger
- pain
- discomfort, such as being wet, too hot or too cold.
Parenting and adjusting to a new baby is rewarding, but it can also bring significant changes and challenges.
If you or your partner are struggling to cope, there is help available. Call and talk to a relative, friend or visit your Child Health Centre, GP, or health professional.
More information:
- Beyond Blue – Pregnancy and new parents or call 1300 22 4636
- Queensland Health – Mental wellbeing during pregnancy
- Perinatal Anxiety and Depression Australia (PANDA) or call 1300 726 306
When will my baby sleep through the night?
Most baby’s wake and feed at night until about six months of age.
There is a large variation of what is ‘normal’. Prolactin (milk making hormone) levels are highest at night, so night feeds are important to ensure adequate stimulation and milk removal from the breast.
Night feeds are important because they:
- provide up to one third of a baby's nutritional needs in a 24 hour period
- help to maintain your breastmilk supply
- can help to prevent engorgement (full and painful breasts)
- can help delay ovulation (return of period)
- can help mothers and babies relax and feel drowsy, due to the hormone cholecystokinin.
-
Important points about breastfeeding
- No formula can ever have the same ingredients as breastmilk.
- Breastmilk has ‘live’ factors in it that protect against illness.
- Breastfed babies are at lower risk of SIDS.
- Starting solids at around six months of age (with no foods or other drinks before this) will make babies less likely to develop illnesses.
- Babies who are given food earlier than six months of age are not any more likely to sleep through the night.
- Breast milk is approximately 87% water. Breastfed babies don’t require any water, even in hot weather, until around six months of age.
- Feeding 8–12 times in a 24-hour period is normal for breastfed babies.
- When babies have growth spurts (fussy days) they seem to feed constantly.
- Mothers are encouraged to eat a healthy, well balanced diet. There are no foods that breastfeeding women should avoid.
- Drinking more fluids or eating certain foods does not change milk supply.
- It is recommended that breastfed babies do not use dummies for the first four to six weeks.
- Substituting a breastfeed with a bottle on a regular basis can reduce your milk supply.
- Seeking breastfeeding advice or support from a health professional is recommended.
More information:
- Queensland Clinical Guidelines parent information – Breastfeeding your baby
- Australian Breastfeeding Association – Breastfeeding Information
- Queensland Health – Babies and Toddlers
- Queensland Health – Breastfeeding
Next section: Expressing breastmilk
-
Expressing breastmilk
-
Expressing and storing breastmilk

Almost all mothers in Australia (98%) express milk at some time for their baby in the first six months.
It is important you know how to express milk by the time you are discharged from hospital.
Reasons why some mothers will have to express:
- baby is sick or preterm
- mother and baby are separated
- mother is returning to work
- to increase milk supply
- if breasts are uncomfortable or full.
There are three methods of expressing breastmilk:
- hand
- hand pump
- electric pump.
Encouraging your let-down reflex
Whichever way you are expressing, it is important that milk 'lets-down' so that a good quantity of milk is obtained.
Ways to encourage your let-down reflex:
- sit comfortably
- relax – practice deep breathing exercises
- listen to relaxing music
- warmth – apply gentle heat from a warm face washer
- massage – lightly massage your breasts towards the nipple before and during expressing
- stimulation – gently roll your nipples between your fingers
- thinking of your baby or looking at a photo of them, while expressing.
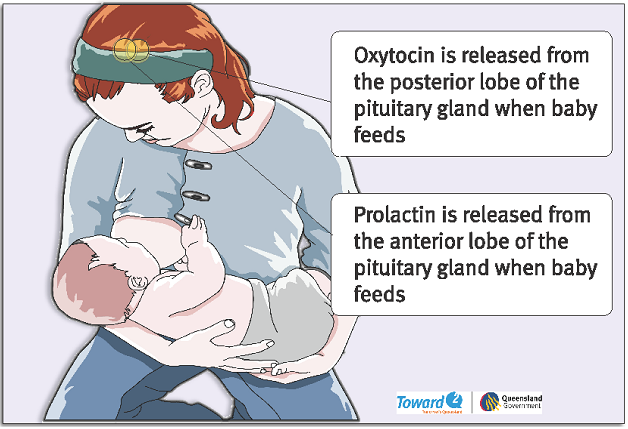
-
Steps for expressing milk by hand
Wash hands with soap and warm water and thoroughly dry. Hold a clean plastic cup/dish under the breast to collect the milk.
1. Gently massage the breast – start from the top of the breast and stroke towards the nipple, massage the underside and repeat several times to ensure that the whole breast is massaged.
1
2. Place thumb and finger diagonally opposite each other on the edge of the areola. Gently press inward towards the centre of the breast, squeezing the finger and thumb together.
2
3. & 4. Repeat with a rhythmic rolling movement, feeling for the milk sinuses – the fingers should not slide over or pinch the skin. Once the milk flow has stopped, move the fingers around the nipple and press again. Repeat the process on the other breast.
3

4

Milk ejection (let down)

-
Storage of expressed breastmilk (EBM)
Look in your baby’s Personal health record (red book) for more information.
Thawing and warming of breast milk
- Frozen EBM must be warmed quickly but NOT in boiling water, as the milk will curdle.
- DO NOT leave EBM to stand at room temperature to thaw.
- Place the container under running cold water. Gradually make the water warmer until the milk becomes liquid.
- Warm the container of chilled or thawed EBM in a jug of hot water until it is body temperature.
Breast milk Room temperature Refrigerator Freezer Freshly expressed into a clean container6–8 hours
(26°C or lower)3–5 days
(4°C or lower)- 2 weeks in freezer compartment inside a refrigerator
- 3 months in freezer if separate door
- 6-12 months in deep freezer
Previously frozen, thawed in a fridge4 hours or less
24 hours Do not refreeze Previously frozen, thawed outside a fridge in warm water Completion of feed 4 hours until next feed Do not refreeze Baby has begun feeding Completion of feed
Discard Discard Caution!
- Microwave ovens should NEVER be used to thaw or heat breastmilk. Their safety is unknown and heating is uneven.
- EBM cannot be reheated if your baby does not finish the feed. So warm only a small amount at a time.
- Label all breast milk containers with the date and time breastmilk was expressed. Use the oldest milk first.
Next section: Postnatal care – baby and you
-
Postnatal care – baby and you
-
Baby’s safety and security in hospital
Rooming in
In the postnatal ward, your baby will be in the same room so you can see signs that your baby is hungry, uncomfortable, needs a change or wants a cuddle. We call this ‘rooming in’.
There are many benefits to rooming in:
- you can cuddle your baby whenever you want
- you can breastfeed when your baby shows feeding signs
- you can get to know your baby before you go home.
Bed sharing in hospital
Sharing your bed with your baby for the purpose of sleeping is not an accepted practice within the hospital environment, as in some circumstances this has been associated with an increased risk of sudden infant death (SIDS) and fatal sleeping accidents.
Please return your baby to the cot after feeding and cuddles. This is especially important when you are very tired and finding it difficult to stay awake.
More information: Red Nose – safe sleeping
Identification
Your baby needs to have two identification bands (usually one on their hand and foot) and a tape identification on their back at all times. Please notify your midwife/nurse immediately if any of these become loose or fall off.
If you are ever separated from your baby, ensure that you and the staff check the identification bands against yours, once you are reunited.
While in hospital, your baby will be identified by your surname. For example, ‘Smith, B/O Sarah Jane’. B/O stands for ‘Baby Of’, and Sarah Jane would be the mum’s first name and middle name. Later, when registering your baby’s birth, you may choose to use either your surname or the father’s surname.
When can I go home?
If you have a normal, uncomplicated vaginal birth, you can expect to be discharged from hospital between six and 24 hours after birth.
If you have an uncomplicated caesarean birth, discharge may be 48–72 hours after birth.
If you are in the postnatal ward you will receive ongoing care and support from the midwives, nurses, medical officers and allied health team. Discharge time can vary depending on the time of birth but is generally 10:00 am.
The midwives will offer discharge information and you will have an opportunity to ask questions before you go home.
-
How do I register my baby’s birth?
After your baby is born, you will be given a birth registration pack, including:
- how to register your baby’s birth
- how to order a birth certificate/extract or commemorative birth certificate.
In the case of same sex female parents, only one parent can be registered as the baby's mother.
More information:
-
Looking after yourself at home
Ways to get support
Practical support
Involve your family and friends. They can provide a network of help for emergencies, babysitting, social activities and ‘time out’ for you.
Personal support
These are people you can talk to about how you are feeling. They may include family, friends and health professionals.
Ways to take care of yourself
- sleep when your baby is sleeping
- limit outside activities and visitors
- drink lots of water and eat healthy foods
- try to get exercise and fresh air every day
- join a breastfeeding or new mothers support group
- talk about your feelings with your partner or others
- let family and friends help with chores.
More information:
- Pregnancy, Birth and Baby helpline or call 1800 882 436
- Child Health Service (Children’s Health Queensland)
- Parents’ Groups
- Ryan's Rule
- Red Nose Grief and Loss Support – miscarriage, stillbirth and newborn death support
-
Your physical health and wellbeing
Your breasts
Many women experience some difficulties when establishing breastfeeding, most are minor and can be overcome by advice, assistance and support.
On the third or fourth day after your baby is born, your breasts may become fuller as the milk flow increases.
Your midwife, child health nurse or a lactation consultant will be happy to help or you may like to review the breastfeeding section or contact:
- 13 HEALTH (13 43 25 84)
- Australian Breastfeeding Association Helpline 1800 mum 2 mum (1800 686 2 686)
Your abdomen
Your abdomen will probably be quite ‘baggy’ and soft after birth. Despite birthing your baby, the placenta and a lot of fluid, you’ll still be quite a lot bigger than you were before pregnancy. This is partly because your muscles have stretched. If you eat a balanced diet and get some exercise, your shape should soon return to normal.
Breastfeeding helps because it makes the uterus contract. Because of this, you may sometimes feel a painful ‘twinge’ in your stomach or period-type pain while you are breastfeeding. These are known as ‘afterbirth’ pains. These usually settle after a few days.
Your bladder
After having a baby, it’s quite common to leak urine accidentally if you laugh, cough or move suddenly. Pelvic floor exercises can help prevent this. If the problem lasts for more than three months, see your GP, who may refer you to a physiotherapist.
More information: Continence Foundation of Australia – Pregnancy
Bleeding after your birth
After your birth, you will bleed from your vagina. This will be quite heavy at first, which is why you will need super-absorbent sanitary pads. Do not use tampons until after your six week postnatal check, as they can cause infections.
During a breastfeed, you may notice that the bleeding is heavier along with ‘afterbirth’ pains.
Gradually the bleeding will become a brownish colour and may continue for some weeks, getting less and less until it stops.
Be alert!
If the amount of bleeding suddenly increases, call 13 HEALTH (13 43 25 84) to discuss what is normal and what may be an emergency. If you find you are losing blood in large clots, you should save your sanitary pads to show the midwife or doctor.
Haemorrhoids
Haemorrhoids are very common after birth and usually disappear within a few days.
Eat plenty of fresh fruit, vegetables, salad, wholegrain bread and cereals, and drink plenty of water. This should make bowel movements easier and less painful. Do not push or strain because this will make the haemorrhoids worse.
Always see your GP if you are concerned.
Stitches
If you have stitches after tearing in your perineum (the area between the vagina and anus) or an episiotomy (where the midwife or doctor has cut the perineum so your baby can be birthed more easily), make sure you shower with plain warm water. After showering, dry yourself carefully. In the first few days, remember to sit down gently and lie on your side rather than on your back.
If the stitches are sore and uncomfortable, tell your midwife as they may be able to recommend treatment.
Painkillers will also help. If you’re breastfeeding, check with your midwife, doctor or pharmacist before you buy over-the-counter products, such as ibuprofen or paracetamol. The stitches do not need to be removed—they will dissolve by the time the area has healed.
Rhesus negative mothers
If your blood group is Rhesus negative, blood samples will be taken after the birth to see whether your baby is Rhesus positive.
You may need an injection to protect your next baby from anaemia. If so, the injection should be given within 72 hours of your baby being born.
Check with one of the doctors or midwives about what should happen in your case.
More information: Queensland Clinical Guidelines parent information – RhD negative blood type in pregnancy
Tests and immunisations for you
After you’ve had your baby, you’ll be offered some checks and immunisations.
Rubella
If you were not immune to rubella (German measles) when tested early in your pregnancy, you will usually be offered the MMR (measles, mumps and rubella) vaccine by your midwife before you leave the hospital, or shortly afterwards by your doctor.
Avoid getting pregnant again for at least one month after the injection.
Family planning / contraception
The return of a menstrual cycle is different for every woman.
Even if you are exclusively breastfeeding, you can start ovulating. That means you can get pregnant again without even knowing that it has happened.
Ask your doctor about your family planning options and if they are compatible with breastfeeding.
Family planning advice and counselling services can be accessed through your GP, women’s health professionals, and True Relationships and Reproductive Health.
Postnatal exercises
Postnatal exercises will help to tone the muscles of your pelvic floor and abdominal muscles (tummy). They will also get you moving and feeling fitter.
Ask your midwife or physiotherapist for postnatal class information.
Recommendations about smoking, drinking alcohol and caffeine while breastfeeding
Review the information in the breastfeeding section .
-
Emotional health after baby
During pregnancy and after baby is born, most women experience a range of emotions. It’s normal to feel some worry during pregnancy and when having a baby. However, if you feel worrying thoughts are becoming a regular part of life, it can help to talk about any concerns with your doctor, partner or a close friend.
It is important to let someone know if you (or your partner) are:
- feeling low, anxious or tense very often
- feeling guilty
- feeling that things are hopeless
- not enjoying things you normally do
- crying all the time
- irritable
- finding it hard to sleep, concentrate or make decisions
- wanting to harm yourself.
Depression and anxiety can occur at any time in your life and can often come to the surface with major events like pregnancy or having a baby.
It is important to keep a check on how you are feeling emotionally and discuss any concerns with your health care professional.
For more information and support:
- Pregnancy, Birth and Baby helpline: 1800 882 436
- Beyond Blue – Pregnancy and new parents: 1300 22 4636
- Perinatal Anxiety and Depression Australia (PANDA): 1300 726 306
- MUMspace – support for the emotional health of new mums, at every step.
- Lifeline: 13 11 14
- Mensline Australia: 1300 78 99 78
- Sane Australia Helpline: 1800 18 7263
- White Cloud Foundation: 1300 702 926
- Black Dog Institute
How can partners help?
Partners can:
- deflect negative comments from friends and relatives
- help calm a fussy baby
- bring the new mother food and drink while she is feeding baby
- tell her she is doing a great job.
-
More information
- Vitamin K at birth – Pregnancy, Birth and Baby
- Immunisation for your child – Pregnancy, Birth and Baby
- Jaundice in newborns – Raising Children Network
- Tummy time – Red Nose
Aboriginal and Torres Strait Islander parents
- Aboriginal and Torres Strait Islander parents – Raising Children Network
Maori and Pacific Islander parents
Good Start to life – Children’s Health Queensland
Multicultural resources
- Languages other than English: resources – Raising Children Network
- Multicultural nutrition resources: Infant feeding for African communities – Metro South Hospital and Health Service
How to wrap your baby
- Wrapping a baby: in pictures – Raising Children Network
- How to wrap a baby (video) – Raising Children Network
- Safe wrapping – Red Nose
Safe bathing for newborns and babies
- Bathing a newborn: in pictures – Raising Children Network
- Bathing a newborn safely (video) – Raising Children Network
Sleep and settling
- How to settle a crying baby (video) – Raising Children Network
- Safe sleeping – Red Nose
Next section: Key words
-
Key words
-
Terms and abbreviations
See your Pregnancy Health Record for a list of terms and abbreviations you may see during your pregnancy.
A
Afterbirth
The placenta. It provides the baby with food and oxygen. It’s attached to your baby by the umbilical cord.
Amniotic fluid
The liquid the baby floats in inside the uterus. Sometimes called ‘the waters’.
Amniotic sac
The bag holding the fluid and the baby inside the uterus.
Amniotomy
A midwife or doctor breaks the amniotic sac which holds the fluid and the baby inside the uterus.
Anaesthetist
A doctor who specialises in providing pain relief.
Anaemia
A deficiency in the number or quality of red blood cells.
Apnoea
The baby stops breathing and needs help to start again.
Augmentation
Medical treatment which may help labour to progress.
B-C
Birth canal
Vagina
Birth plan
A written plan which says what you would like to happen during labour and birth.
Braxton Hicks contractions
Contractions that some women feel in late pregnancy. They are not labour contractions – more like the body practising for labour.
Breech birth
When the baby is born feet or bottom first.
Caesarean section
An operation to deliver the baby. The doctor cuts the abdomen and uterus open to remove the baby.
Cervix
The neck of the uterus.
Contraction
When the muscles in the uterus (womb) tighten.
E-H
EDD or EDB
Estimated date of delivery (or estimated date of birth), also known as your “due date”.
Epidural
A type of anaesthetic that makes you numb below the waist.
Episiotomy
A surgical cut in the area between the mother’s vagina and anus that may be done during labour.
Fetus
The baby is known as a fetus after about the 12th week of pregnancy.
Forceps
Surgical instruments that fit around the baby’s head. They can be used to help the baby out of the vagina.
Hypertension
High blood pressure.
I-O
Induction
An intervention to start the labour rather than waiting for it to happen naturally.
Internal examination
The doctor or midwife puts two gloved fingers into the vagina to check on the progress of labour.
Intervention
Using a medical treatment or instrument to help in labour or birth (e.g. forceps or an induction).
Midwife
Health professional who cares for women and their babies during pregnancy, labour, birth and the postnatal period.
Neonatal
To do with the first 28 days after birth. ‘Neonatal care’ means care of newborn babies.
Neonatologist
Doctor who specialises in caring for newborn babies especially if the baby is unwell.
Obstetrician
Doctor who specialises in caring for women during pregnancy, labour and birth.
P-S
Paediatrician
Doctor who specialises in caring for babies and children.
Pelvic floor
A group of muscles which supports your uterus, bladder and bowel.
Perineum
The area between the vagina and anus.
Placenta
This provides the baby with food and oxygen while in the uterus. It is attached to the inside of your uterus at one end and at the other to the baby via its umbilical cord. It is also called the afterbirth.
Placenta praevia
When the placenta is close to or covers the cervix.
Postnatal (postpartum period)
The first six weeks after the baby is born.
Postpartum haemorrhage
Heavier than normal bleeding after giving birth.
Pre-eclampsia
Serious condition with symptoms of very high blood pressure, headaches and visual disturbances.
Premature
When a baby is born before the 37th week of pregnancy.
Show
Passing the mucus ‘plug’ which seals the cervix.
Antenatal information, 30 Dec 2024, [https://oss-uat.clients.squiz.net/health/children/pregnancy/antenatal-information]
This document is uncontrolled when printed. Before using the information in this document you should verify the current content on https://oss-uat.clients.squiz.net/health/children/pregnancy/antenatal-information.